Prof. Li Qiang
East Hospital Affiliated To Tongji University School of Medicine
Director of the Center for Respiratory and Critical Care Medicine
Director of the Center for Lung Tumors Clinical Diagnosis
and Treatment
Director of the Department of General Internal Medicine
and Internal Medicine Teaching & Research Section
Disclaimer:
- TXI™ and RDI™ Technologies are not intended to replace histopathological sampling as a means of diagnosis
- The positions and statements made herein by Dr. Qiang, are based on Dr. Qiang’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- The BF-P290 used in this case is not available in the US market at this time nor is there an established time for its release. The safety and effectiveness of this product and or the use of these products has not yet been established in the United States market.
- The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
- Dr Qiang, the authoring physician of this presentation, is a paid consultant(s) to Olympus Corporation
Scope : BF-P290
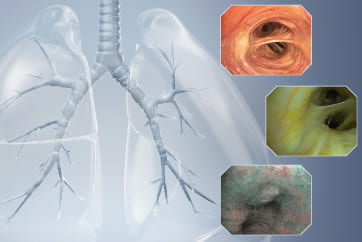
Location : Scarred stenosis of trachea and right main bronchus
Patient Information : Female, 56 years old
Medical History : The patient had a history of bronchial tuberculosis and had undergone temporary bronchial metal stent implantation. After the stent was removed, scarred stenosis of the trachea and right main bronchus was left behind.
1. Tracheal scarred stenosis

(TXI™ Technology mode)
In TXI™ technology mode, the scarred stenotic ring and the surrounding pale scar tissue were clearly shown2. Scar tissue hyperplasia of the right main bronchus

(TXI™ Technology mode)
In TXI™ technology mode, the mucosal scar hyperplasia at the mucosal opening of the right main bronchus was shown, which appeared white or grayish-white, and small blood vessels were seen. The boundary between scar tissue and normal mucosa was clear.3. Endoscopic electro-resection of bronchial stenotic scar tissue
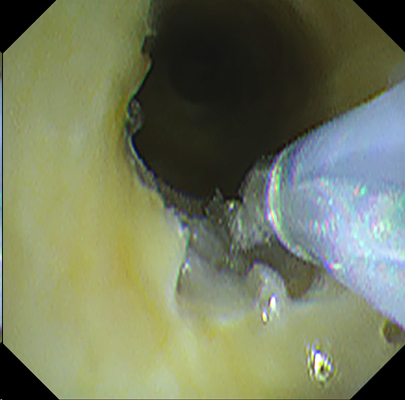
(RDI™ Technology mode)
Electrosurgical excision of bronchial stenotic scar tissue was performed in RDI™ technology mode, which clearly showed that the scar tissue was white and whether bleeding occurred.4. Endoscopic electro-resection of bronchial stenotic scar tissue in WLI mode
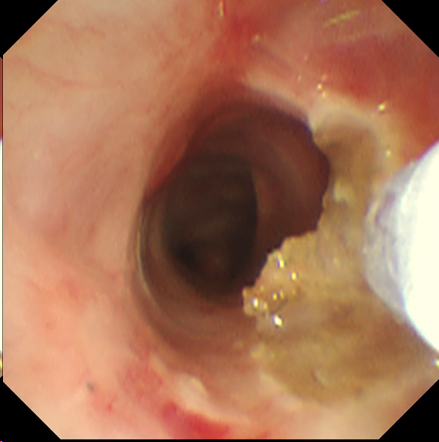
(WLI)
Bronchial scar tissue hyperplasia was difficult to distinguish from normal mucosa in WLI mode, which was not as clear as in TXI™ technology mode, in which scar tissue could be clearly identified from surrounding normal tissue. When no bleeding occurred, WLI mode was almost as good as RDI™ technology mode. Once bleeding occurred, the RDI™ technology mode gave the operator a clearer field of vision and made it easier to determine how to perform endoscopic resection surgery.Endoscopic electro-resection of bronchial stenotic scar tissue was performed in RDI™ technology mode, which clearly showed that the scar tissue was white and whether bleeding occurred.
Overall comment
In TXI™ technology mode, the bronchial scarred stenotic ring and the surrounding pale scar tissue were clearly shown endoscopic electro-resection of bronchial stenotic scar tissue was performed in RDI™ technology mode, which clearly showed that the scar tissue was white and whether bleeding occurred. The RDI™ technology mode gave the operator a clearer field of vision and made it easier to determine how to perform endoscopic resection surgery.
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer
- Content Type