Pancreatobiliary Case 5
Asst. Prof. Dr. Tomislav Bokun
Head, Interventional Gastroenterology Unit
Department of Gastroenterology, Hepatology and Clinical Nutrition
University Hospital Dubrava,
Zagreb, Croatia
Disclaimer:
- NBI™, RDI™ and TXI™ Technologies are not intended to replace histopathological sampling as a means of diagnosis.
- This case study is being furnished to provide examples of NBI™, RDI™, and TXI™ technology use.
- The positions and statements made herein by Dr. Tomislav Bokun are based on Dr. Tomislav Bokun’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
Scope: TJF-Q190V
Organ: Duodenum
Patient information: N/A
Medical history: Suspicion of adenoma growing from intraductally
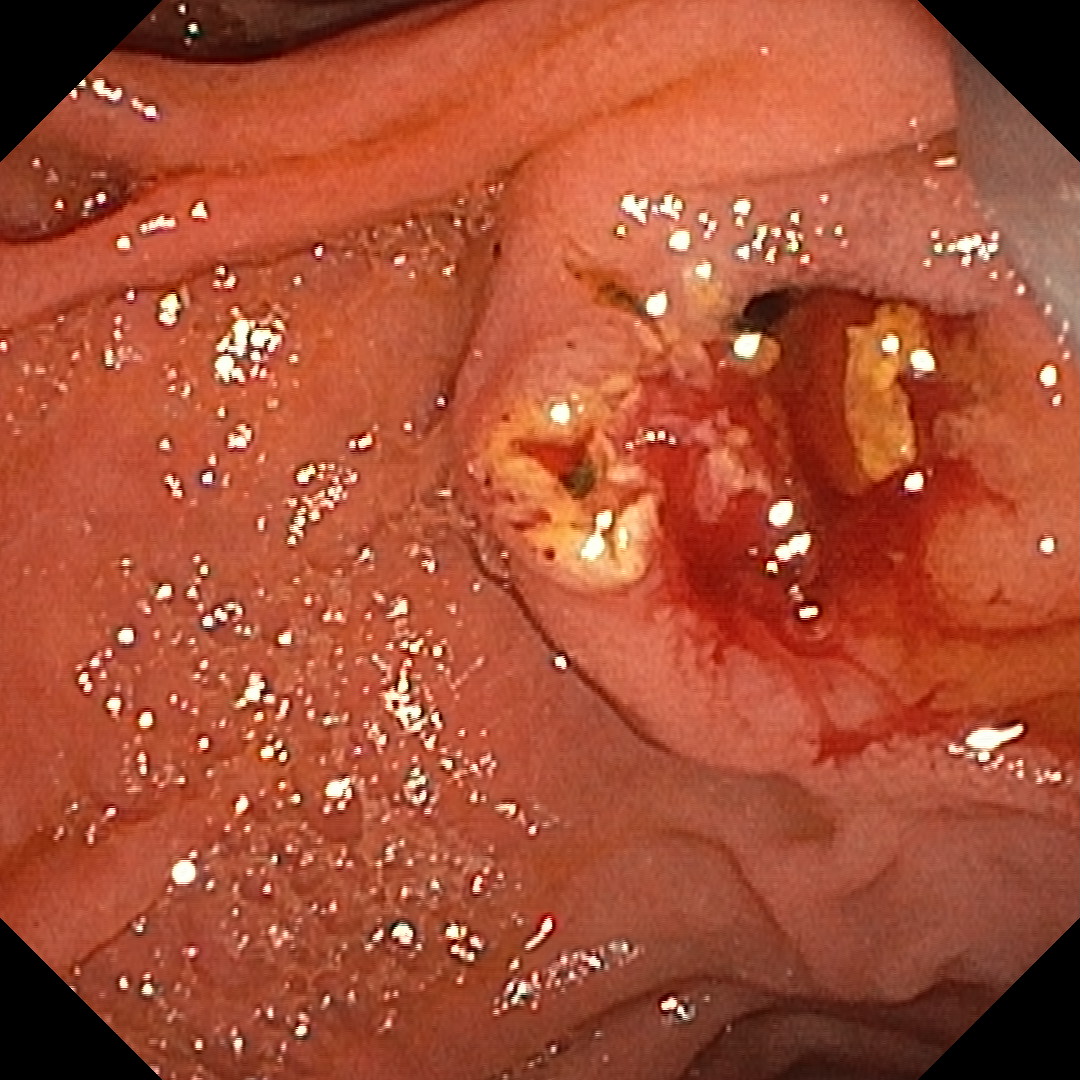
1. Bulging papilla - TXI™ Technology Mode 2

2. After sphincterotmy - WLI
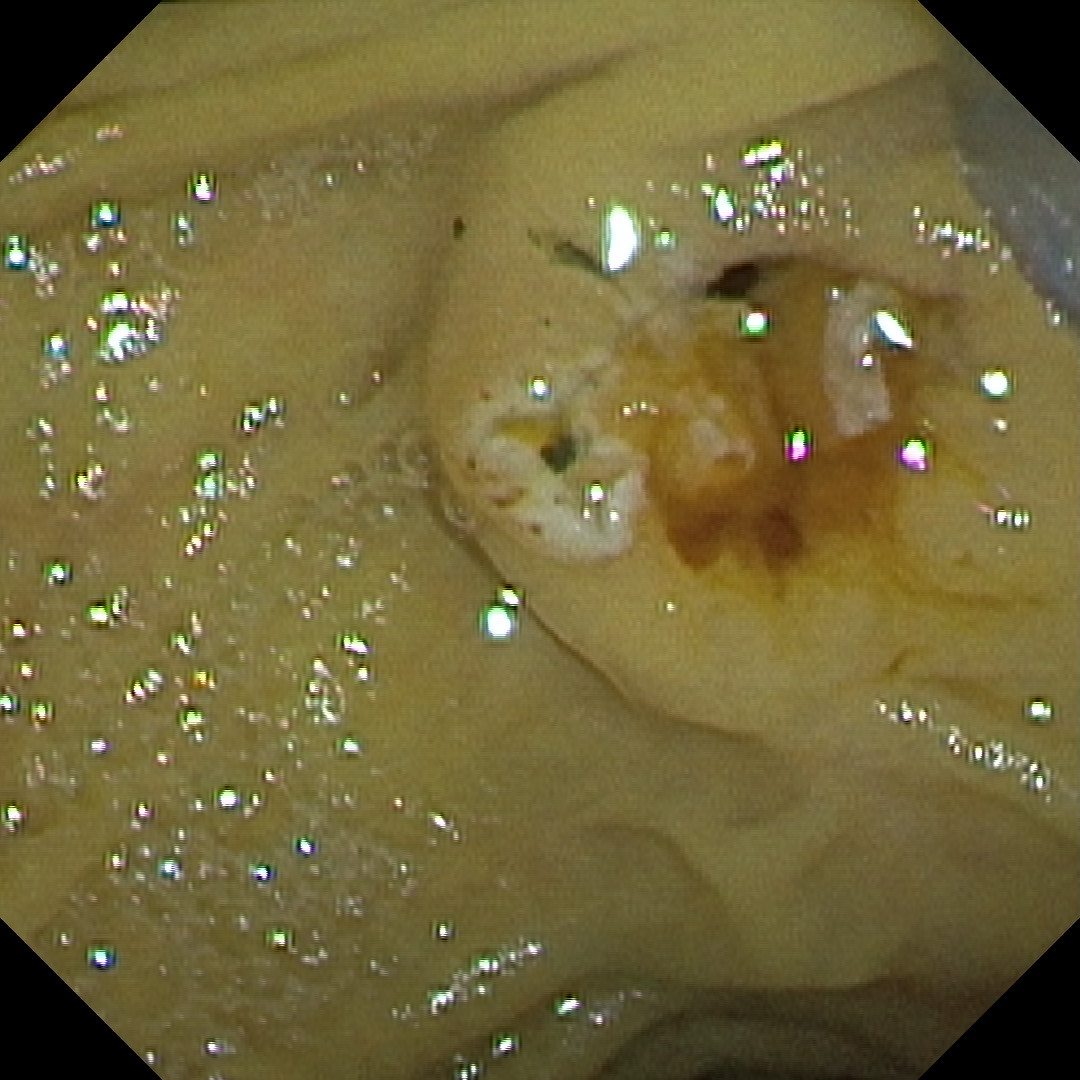
3. Suspicion of postsphincterotomy bleeding - TXI™ Technology Mode 2
4. Suspicion post-sphincterotomy bleeding - WLI
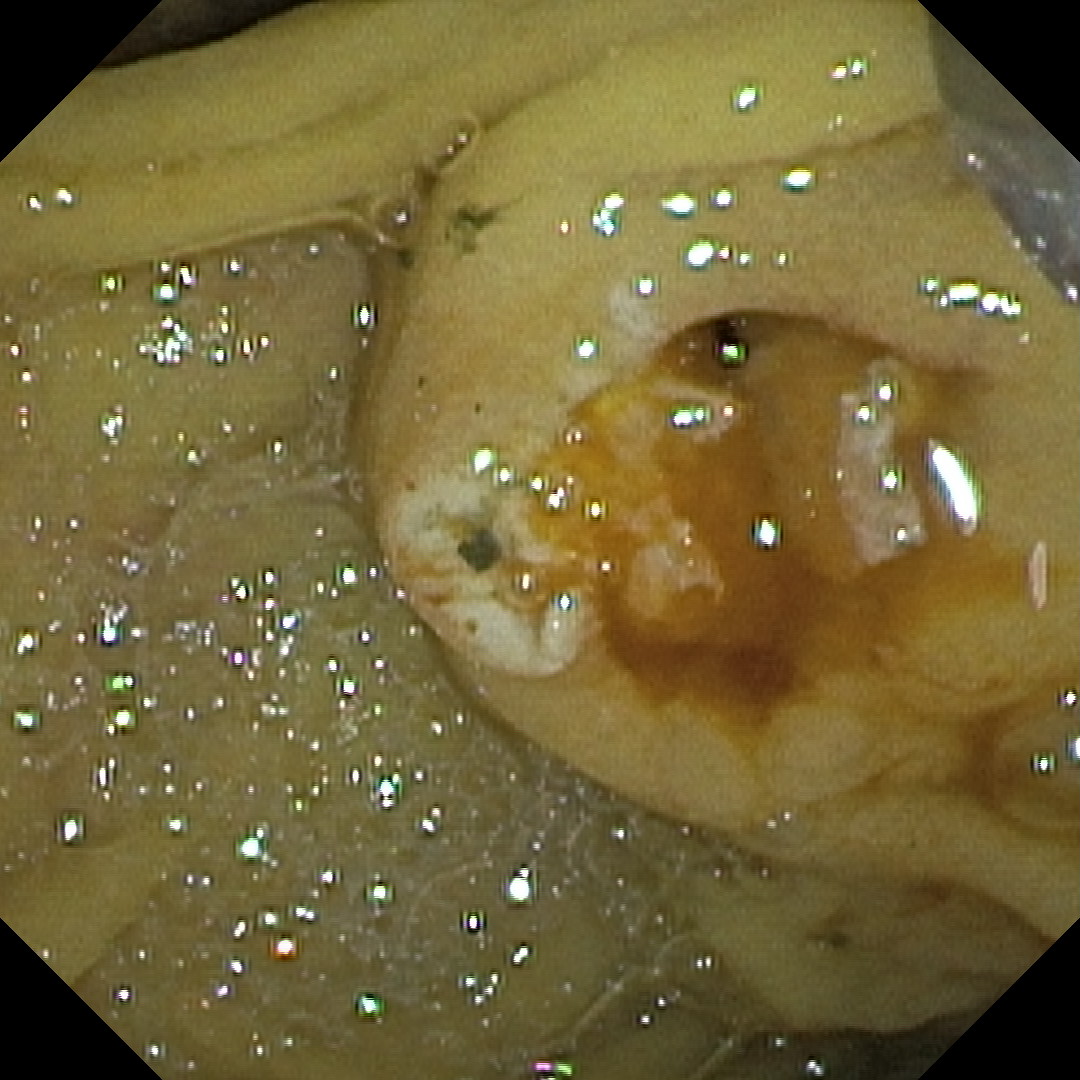
5. Post-sphincterotomy bleeding assessment - RDI™ Technology
6. Post-sphincterotomy bleeding assessment - RDI™ Technology
Case Video
DISCLAIMER: Information regarding competitor products is presented to the best of our knowledge as of the date of presentation. This material does not constitute medical or legal advice and should not be relied upon as such. It should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, warnings and cautions. Techniques, instruments and setting can vary from facility to facility, and it is the clinician’s decision and responsibility in each clinical situation to decide which mode and settings to use.
Overall Comment
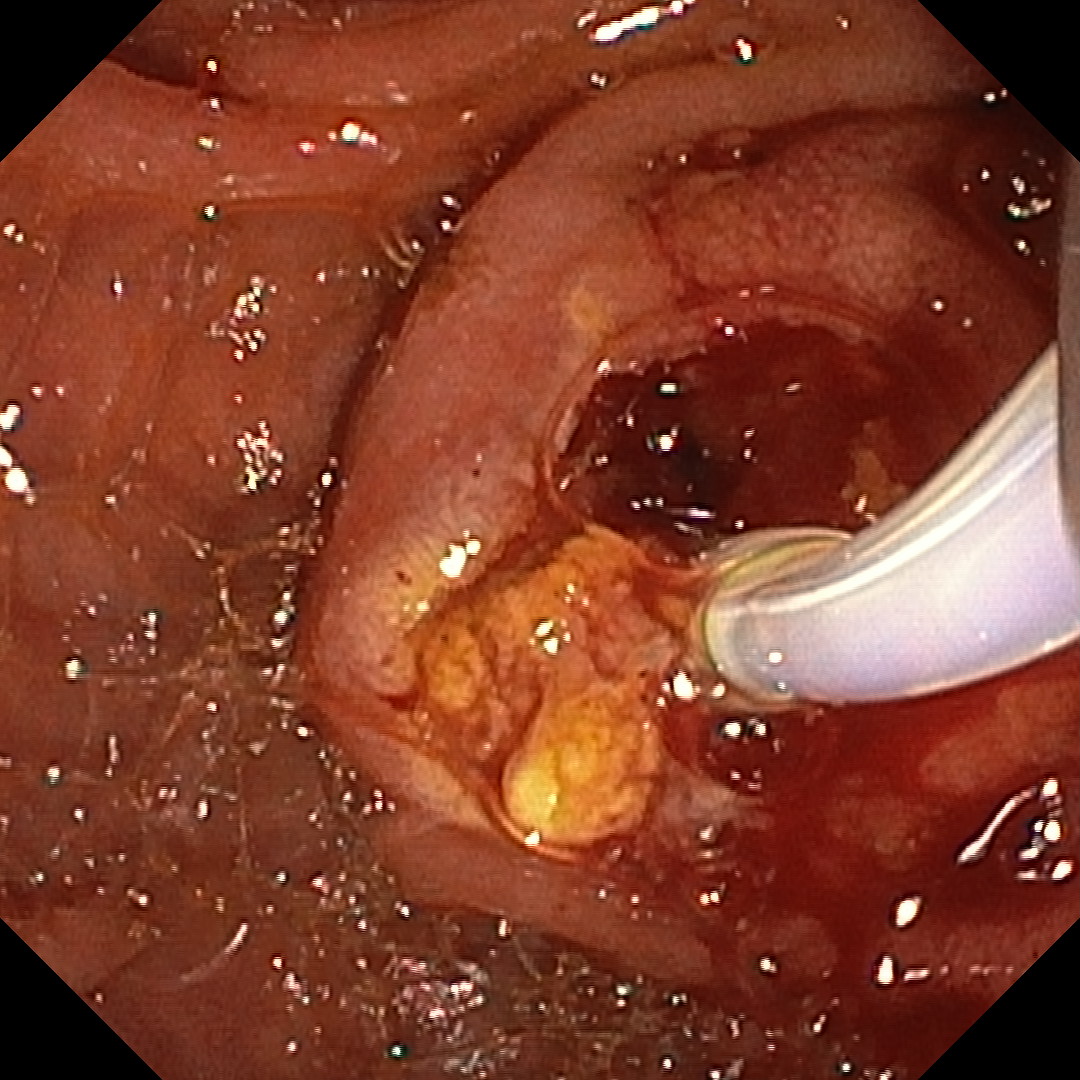
This was a case illustrating how NBI™ technology may aid clinical decision-making. The patient had choledocholithiasis confirmed by EUS; however, the endosonographer described a mildly enlarged papilla with an unclear appearance and raised mild suspicion of organic material in the distal 5 mm of the CBD, referring the patient for duodenoscopy and ERCP.
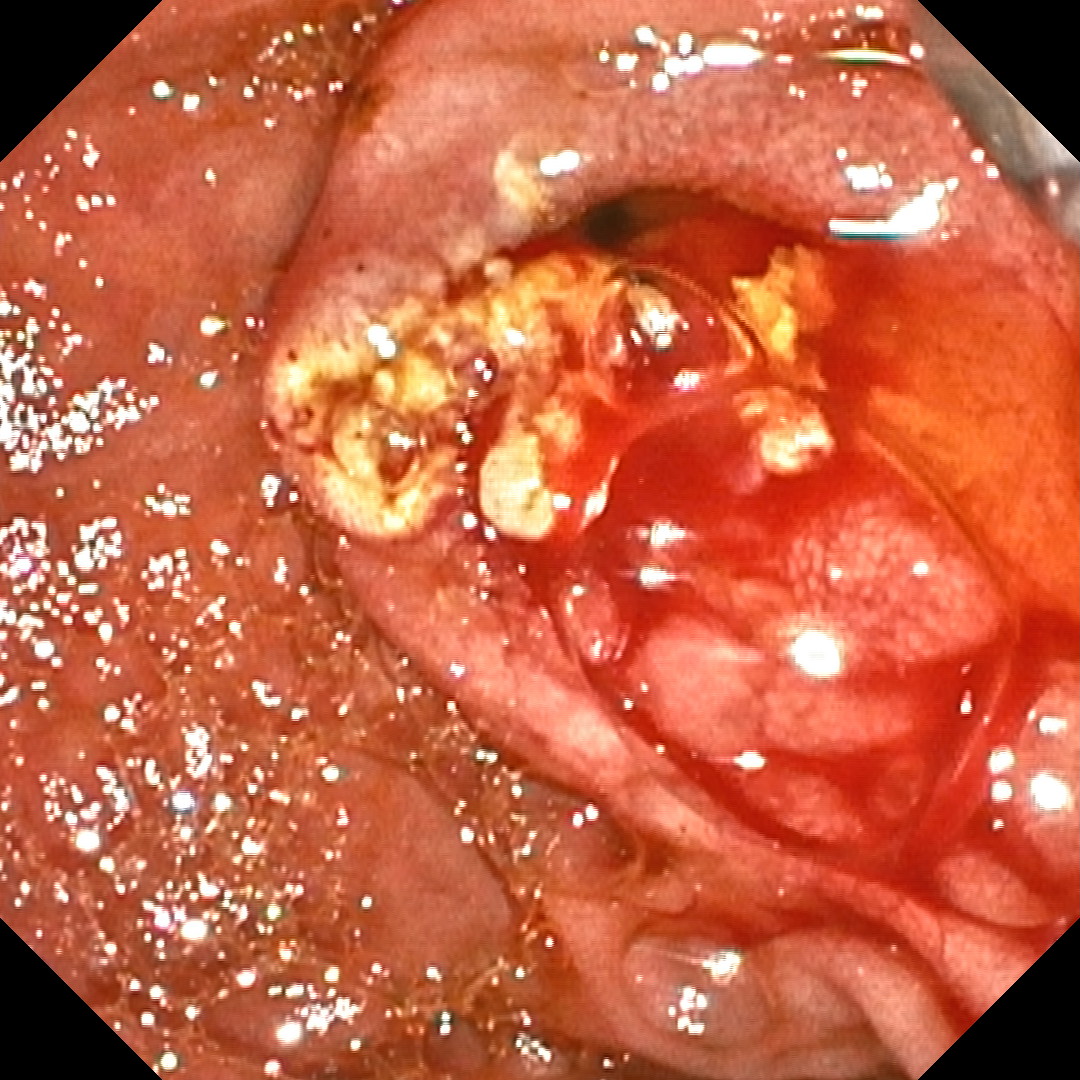
During the procedure I observed a bulging papilla with a small protruding nodule at the orifice, which raised concern for intraductal adenoma given the ambiguous EUS report. The papilla was examined with NBI™ technology; close inspection after manipulation with the sphincterotome showed no neoplastic surface pattern, and the mucosa around the orifice had the same appearance when probed. This reassured me that the findings were likely inflammatory and stone-related rather than an intraductal adenoma.
I proceeded with sphincterotomy. A tiny bleed was seen and was assessed on RDI™ technology. Biopsies were taken from tissue around the orifice, and aspiration with contrast and bile washing across the sphincterotomy line helped demonstrate absence of active bleeding on both WLI and RDI™ technology. Pathohistology later showed inflammation only, with no evidence of neoplasia.
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer