Transnasal Flexible Laryngoscopy – Handling the Endoscope
Insertion of the Endoscope
- Insert the endoscope slowly and with permanent skin contact of the fingers of your left hand with the patient’s nose or cheek. This helps prevent accidental displacement of the endoscope should the patient
move unexpectedly. - When the endoscope tip has passed the anterior nasal cavity, advance the endoscope slowly using just the thumb and index finger.
- Keep finger contact with the nose throughout the examination.
- Be careful not to hurt or to scare the patient with any sudden movements of the endoscope.
- When finishing the examination, withdraw the endoscope slowly and cautiously to avoid hurting the patient.
- During the examination, you should have slackened the flexible shaft of the endoscope into a siphon configuration (see chapter 2.4.3.).


Rotation of the Endoscope
The flexible shaft of the endoscope should not be straight but bowed into a siphon configuration so you can rotate the tip of the endoscope with the fingers of your left hand (A).
Alternatively, you can rotate the tip by rotating the whole endoscope when the flexible shaft is held straight (B).


Flexible Endoscopy – How NOT to Do It
These are fairly common mistakes.





Transnasal Passage and Sequence of Endoscope Positions
Before introducing the endoscope decide which side is more suitable for the nasal passage (e.g. by anterior rhinoscopy).
The choice of side also depends on what you want to see. For instance, the contralateral vocal fold will mostly be exposed better.
For the patient the procedure is more convenient after anesthetization of the nasal cavity.
In some cases decongestant spray is helpful.
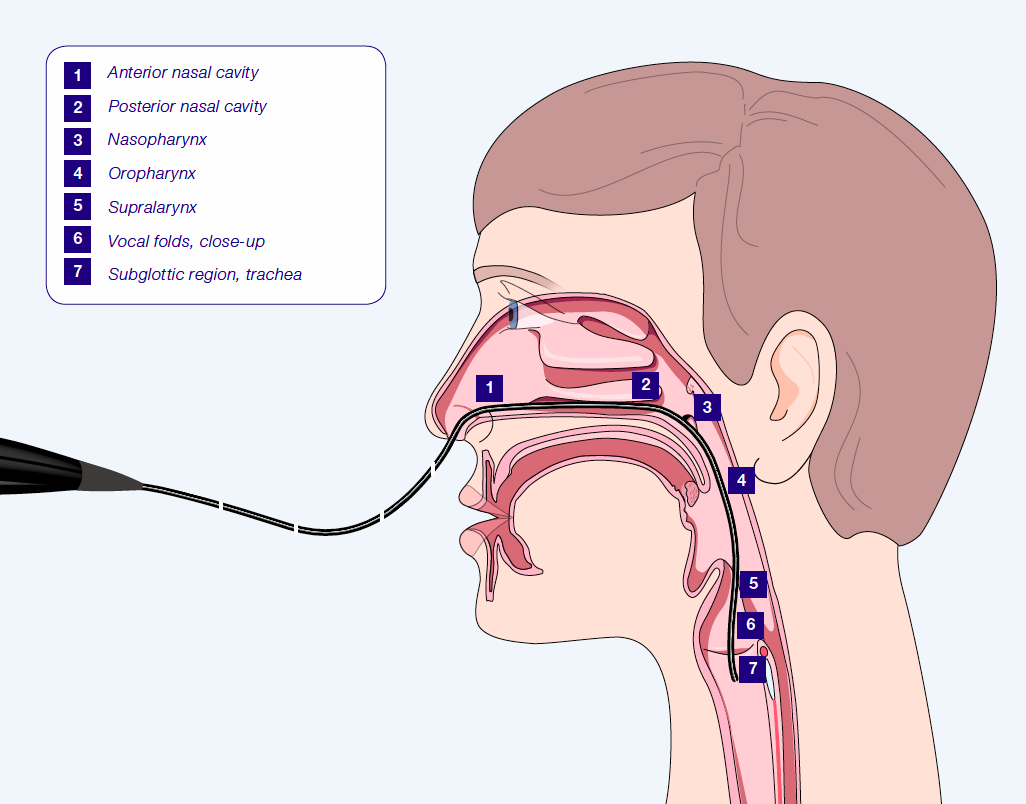
During transnasal endoscopy the nasal cavity, nasopharynx, velopharyngeal function, oro- and hypopharynx, and the larynx can be examined.
For special indications different examination positions might be chosen.
Useful maneuvers in flexible laryngoscopy depending on the position of the of endoscope tip.
Transnasal Passage: Nose and Nasopharynx
Avoid advancing towards the septum – the mucosa of the turbinates will generally yield but the mucosa of the septum does not.
Where the nasal cavity is narrow, try the middle meatus. The two turbinates will generally yield enough space to permit passage of the endoscope. Try the inferior meatal route only when this approach fails.
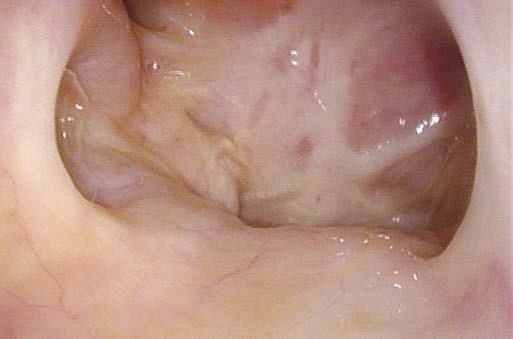
Positions of the Endoscope Tip within the Nasal Cavity




When passing the endoscope into the nasopharynx, ask the patient to breathe through his nose so that the velum relaxes.
When examining velopharyngeal function, ask the patient to swallow or to phonate e.g. “eee” or “coke”.
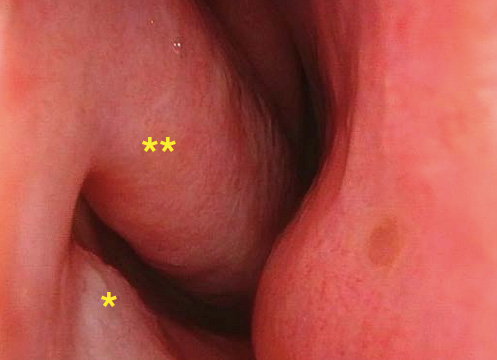
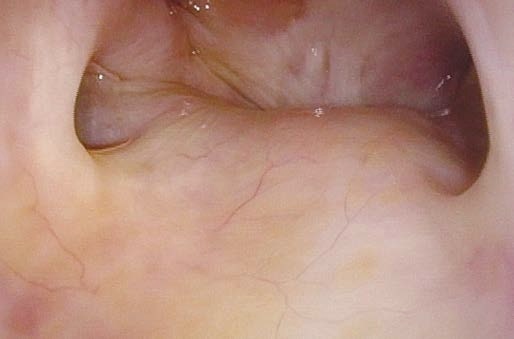
Positions of the Endoscope Tip within the Posterior Nasal Cavity

Transnasal Passage: Oro- and Hypopharynx, Larynx, Trachea
With flexible endoscopy it is possible to evaluate the vocal tract configuration during speaking, singing and special maneuvers.
For assessing the morphology of the vocal folds it is recommended to position the tip of the endoscope very close to the glottis. It is often possible to pass the glottis and have a look at subglottis and trachea.
In case subglottis and trachea are part of the clinical question anesthetize the larynx.
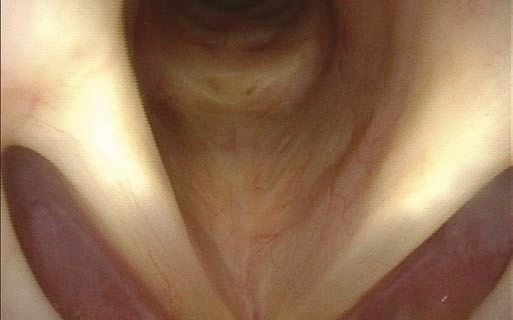
Positions of Endoscope Tip within the Naso-, Oro-, and Hypopharynx and the Larynx







|
Numbers According to Reference Points (see Fig. 4.1.) |
Position of Endoscope | Maneuver | Pay Special Attention to: |
|---|---|---|---|
| 2, 3 | Posterior nasal cavity above velum and nasopharynx | Breathe through nose | Spontaneous movements of velum and upper pharyngeal muscles; velopharyngeal distance |
| Swallow | Velopharyngeal closure, regurgitation | ||
| Articulation of e.g. “coke” | Velopharyngeal contact | ||
| 4 | Oropharynx | Breathing at rest | Spontaneous movements of lower pharyngeal and laryngeal muscles, acute signs of VCD, tremor, dystonia |
| Repeated phonation of “eee” following by sniffing | Mobility of arytenoids | ||
| Throat-clearing, coughing, laughing | Nonphonatory rapid movements, diadochokinesis of arytenoids | ||
| Counting softly and with habitual loudness level | Vocal tract configuration | ||
| Oro- and hypopharynx | Examination of swallowing | Intraoral control of bolus, pre-, intra-, and postdeglutitive laryngeal penetration/aspiration | |
| 4, 5, 6 | Oro- and hypopharynx, larynx | Forced and rapid inspiration | Extent of edema Pedunculated lesions Stability of arytenoid complex |
| Inspiratory phonation | Pliability of mucosa Extent of edema, pedunculated lesions | ||
| Stroboscopy: 10 sec. “eee” with habitual loudness level and pitch | Phonatory involvement of mucosal wave, pliability of mucosa, regularity of vibration | ||
| 6, 7 | Position close to glottis or subglottis / in trachea | Long nasal inspiration (dipping maneuver) | Fine structures of vocal fold Morphology of Morgagni’s ventricle, anterior commissure, subglottis, trachea |
| 7 (in case of tracheostomy) |
Transstomal and intratracheal | Breathing at rest | Visualization of glottis transstomal Visualization of trachea Cannula-induced ulcers |
| Phonation | Respiratory mobility | ||
| Examination of swallowing with transstomal visualization | Aspiration (turn endoscope upwards to inspect glottis and downwards to inspect lower trachea) |
Table 4.2.: Flexible laryngoscopy: Useful maneuvers depending on position of endoscope (see Fig. 4.1)
- Content Type