Yo Kishimoto, M.D., Ph.D.
Associate Professor,
Department of Otolaryngology-Head and Neck Surgery,
Graduate School of Medicine, Kyoto University, Kyoto, Japan
Disclaimer:
- NBI™ Technology is not intended to replace histopathological sampling as a means of diagnosis
- The positions and statements made herein by Dr. Kishimoto are based on Dr. Kishimoto’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- The VISERA S™ Video System Center is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU).
- Unless otherwise noted, the visual media and clinical images contained within this material have been provided by Dr. Kishimoto. All rights reserved.
1. Importance of Endoscopic Examination in Head and Neck Practice
Endoscopic examination plays a central role in head and neck practice, with white-light imaging serving as the fundamental modality. Using white-light observation, most elevated lesions, including vocal fold polyps, can often be visually identified and clinically assessed. Recent technological advances have markedly improved image quality, enabling more detailed visualization and lesion characterization. Furthermore, the ability to digitally record endoscopic findings has become an important tool in contemporary head and neck practice.
However, the early detection of superficial laryngopharyngeal carcinoma, which has been increasing in recent years, remains challenging with white-light observation alone. In addition, evaluation of vocal fold vibration in voice disorders and assessment of tumor depth in glottic carcinoma are not possible using white-light imaging alone. These evaluations may be supported through adjunctive imaging technologies such as NBI™ (Narrow Band Imaging™) technology and stroboscopic observation, respectively. Such advanced visualization is clinically essential, as they directly contribute to appropriate treatment selection and improved therapeutic outcomes.
With conventional otolaryngologic endoscopes, NBI™ technology observation has often been limited by lower resolution compared with gastrointestinal endoscopes and by frequent halation due to surface reflection, which can complicate diagnosis. Similarly, stroboscopic observation has frequently suffered from insufficient illumination, making accurate assessment of mucosal vibration difficult, particularly in patients with strong reflectivity where close observation is challenging.
Moreover, when NBI™ technology for microvascular assessment and stroboscopy for depth evaluation are used in combination for the diagnosis of early glottic carcinoma, switching between different light sources is required, resulting in procedural complexity for both healthcare providers and patients.
2. Features of VISERA S OTV-S500
The VISERA™ S OTV-S500 light-source-integrated endoscopic system enables the use of a stroboscopic observation mode through software upgrades via a portable memory port. This system allows one-touch switching between NBI™ technology and stroboscopic observation.
Functionally, the system employs narrow-spectrum violet LEDs in addition to white LEDs, thereby supporting contrast-enhanced visualization during NBI™ technology observation. Noise reduction is achieved through frame accumulation and image processing techniques. Furthermore, increased luminous intensity enabled by high-current output, combined with the integrated light-source design, supports integrated in-system image processing. This configuration suppresses flicker caused by mismatches between the camera shutter speed and the light source flashing cycle.
Another notable feature of the system is its compact and lightweight design. The main unit measures 308 mm in width, 157 mm in height, and 461 mm in depth, with a total weight of only 10.6 kg, supporting transportation and installation across clinical environments.
3. Clinical Utility of the VISERA™ S OTV-S500 System in Early Detection and Extent Assessment of Superficial Head and Neck Cancer and High-Grade Dysplasia
Case 1: Oropharyngeal Squamous Cell Carcinoma (cT1N0M0)
Disclaimer: Representative clinical case shown for educational purposes. Individual findings and visualization may vary
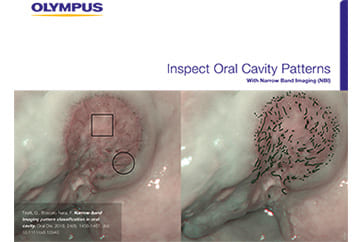
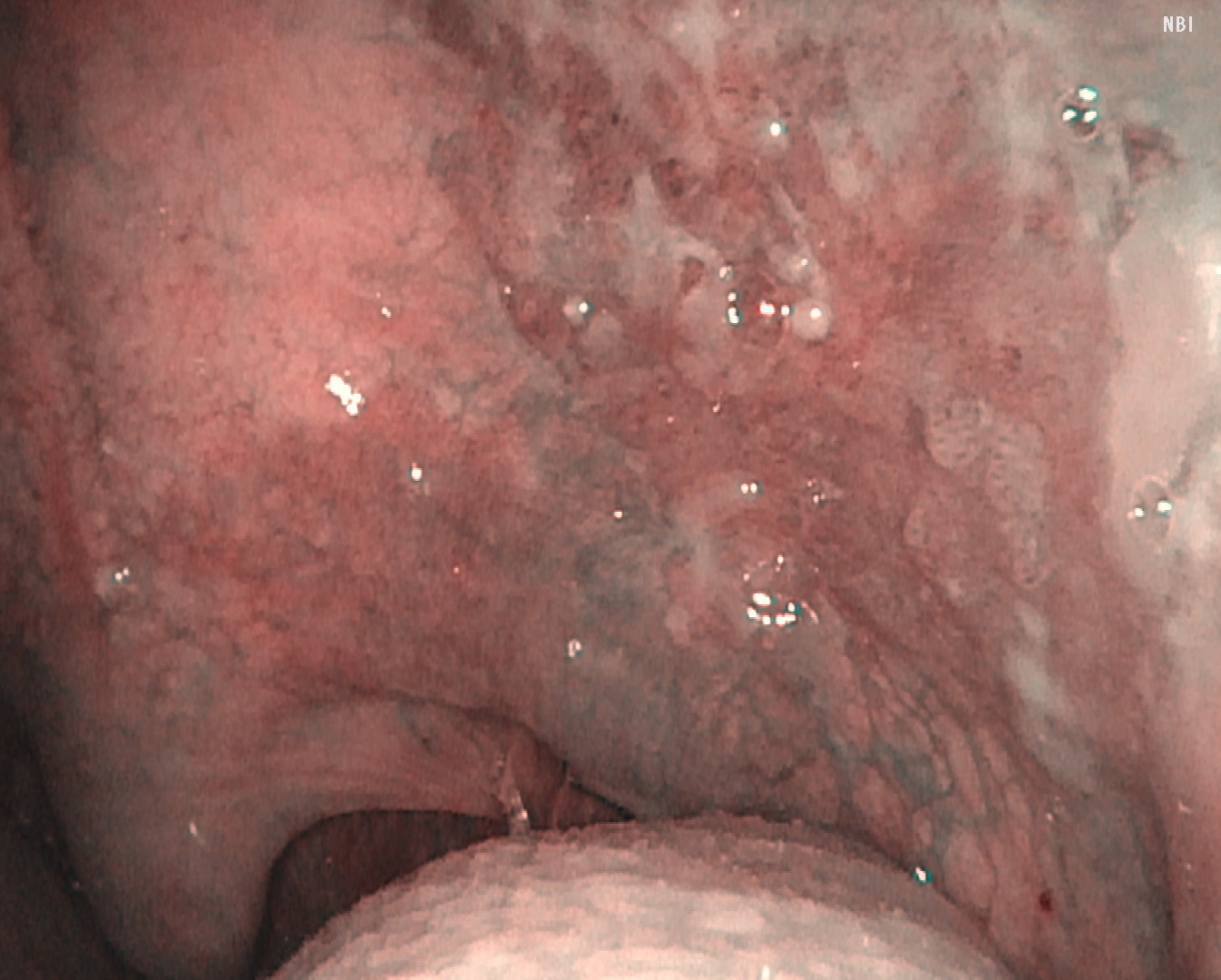
White-light observation revealed an erythematous lesion with an irregular surface extending from the left soft palate to the anterior palatine arch; however, visual assessment of lesion extent was challenging. NBI™ technology observation demonstrated a well-demarcated brownish area with proliferative atypical microvessels. Using the VISERA™ S OTV-S500 system provided contrast-enhanced visualization in this case, and lesion margins appeared more clearly visualized.
NBI™ Technology Image
Video System Center: VISERA ELITE™ OTV-S190 System
Video Rhinolaryngoscope: ENF-VH
Representative white-light and NBI™ images from the same clinical case for visualization purposes.

White Light Image
Video System Center: VISERA™ S OTV-S500 System
Video Rhinolaryngoscope: ENF-VH
NBI™ Technology Image
Video System Center: VISERA™ S OTV-S500 System
Video Rhinolaryngoscope: ENF-VH
Case 2: Hypopharyngeal High-Grade Dysplasia
Disclaimer: Representative clinical case shown for educational purposes. Individual findings and visualization may vary.
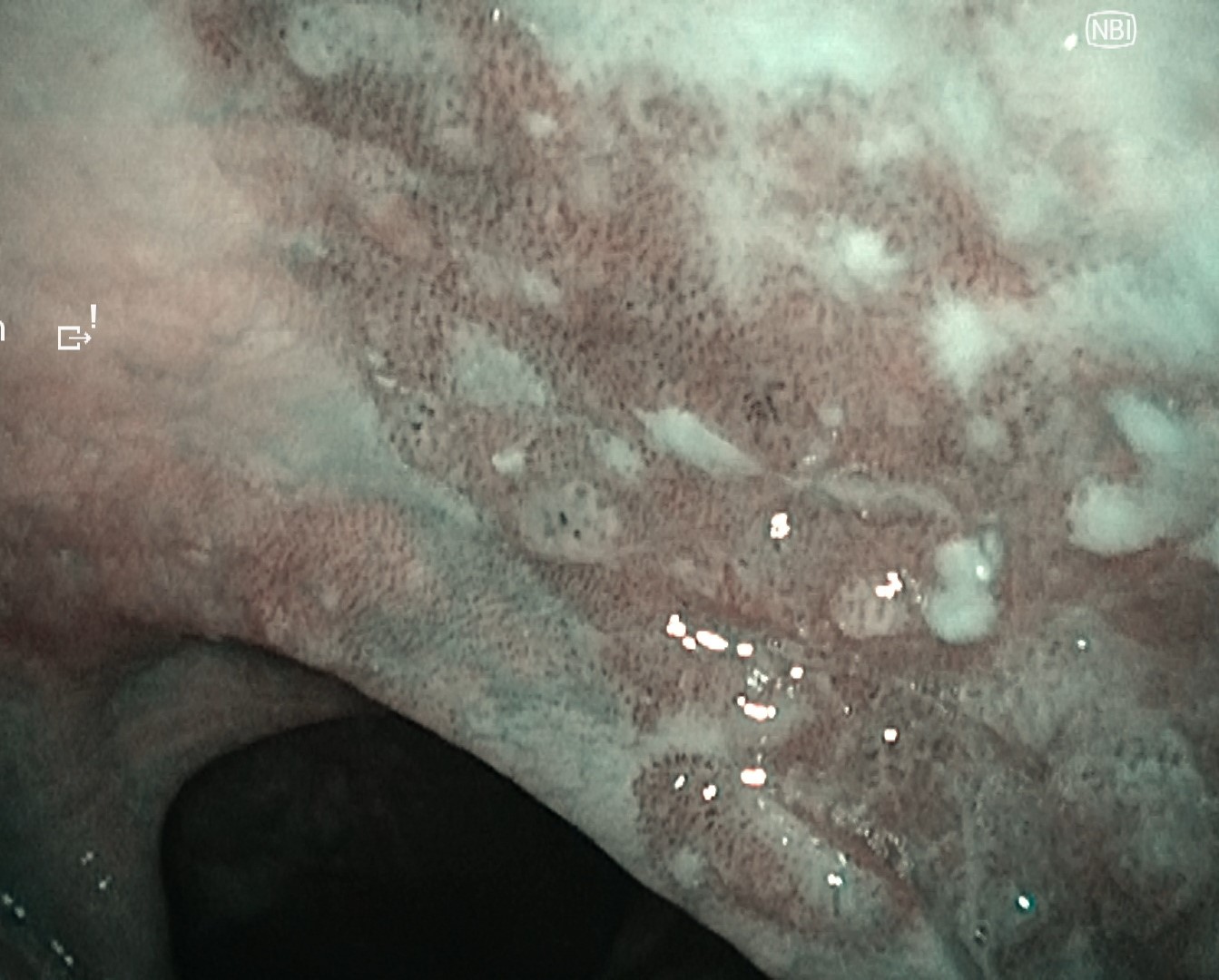
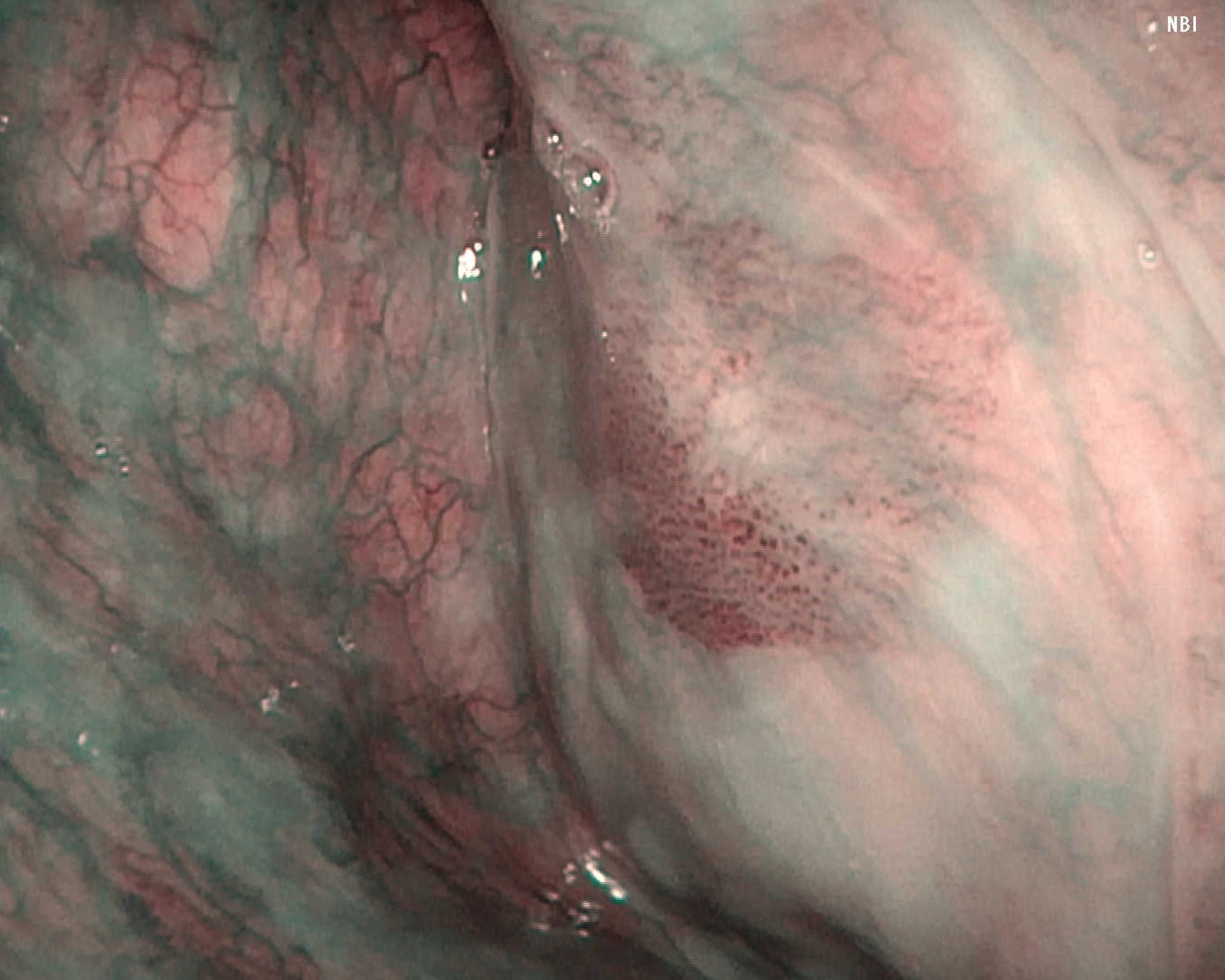
Following observation of the hypopharynx using the modified Killian method, slight erythema was noted on the mucosa of the right pyriform sinus. NBI™ technology observation revealed a clearly demarcated brownish area with atypical microvascular proliferation at the same site. Using the VISERA™ S OTV-S500 system, lesion characteristics were visualized in this representative case.
Representative white-light and NBI™ technology images acquired from the same lesion during clinical evaluation. Visualization may vary by case.
White Light Image
Video System Center: VISERA ELITE™ OTV-S190 System
Video Rhinolaryngoscope: ENF-VH
NBI™ Technology Image
Video System Center: VISERA ELITE™ OTV-S190 System
Video Rhinolaryngoscope: ENF-VH

White Light Image
Video System Center: VISERA™ S OTV-S500 System
Video Rhinolaryngoscope: ENF-VH
NBI™ Technology Image
Video System Center: VISERA™ S OTV-S500 System
Video Rhinolaryngoscope: ENF-VH
Case 3: Hypopharyngeal High-Grade Dysplasia
Disclaimer: Representative clinical case shown for educational purposes. Individual findings and visualization may vary.
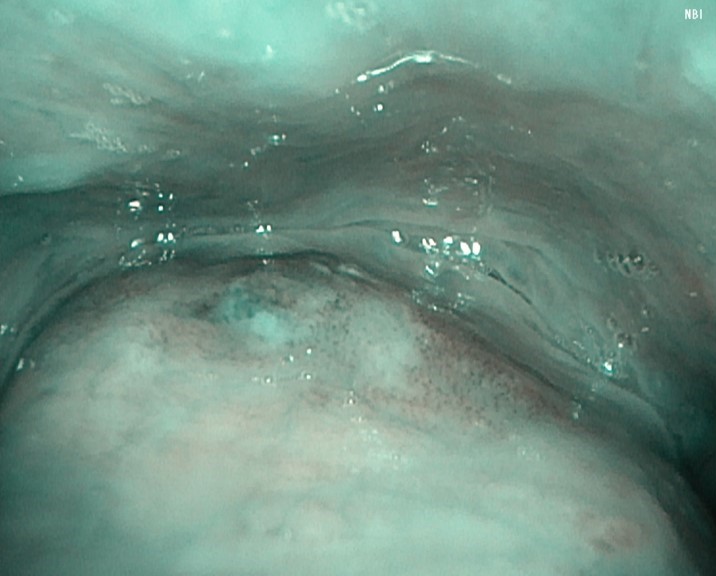
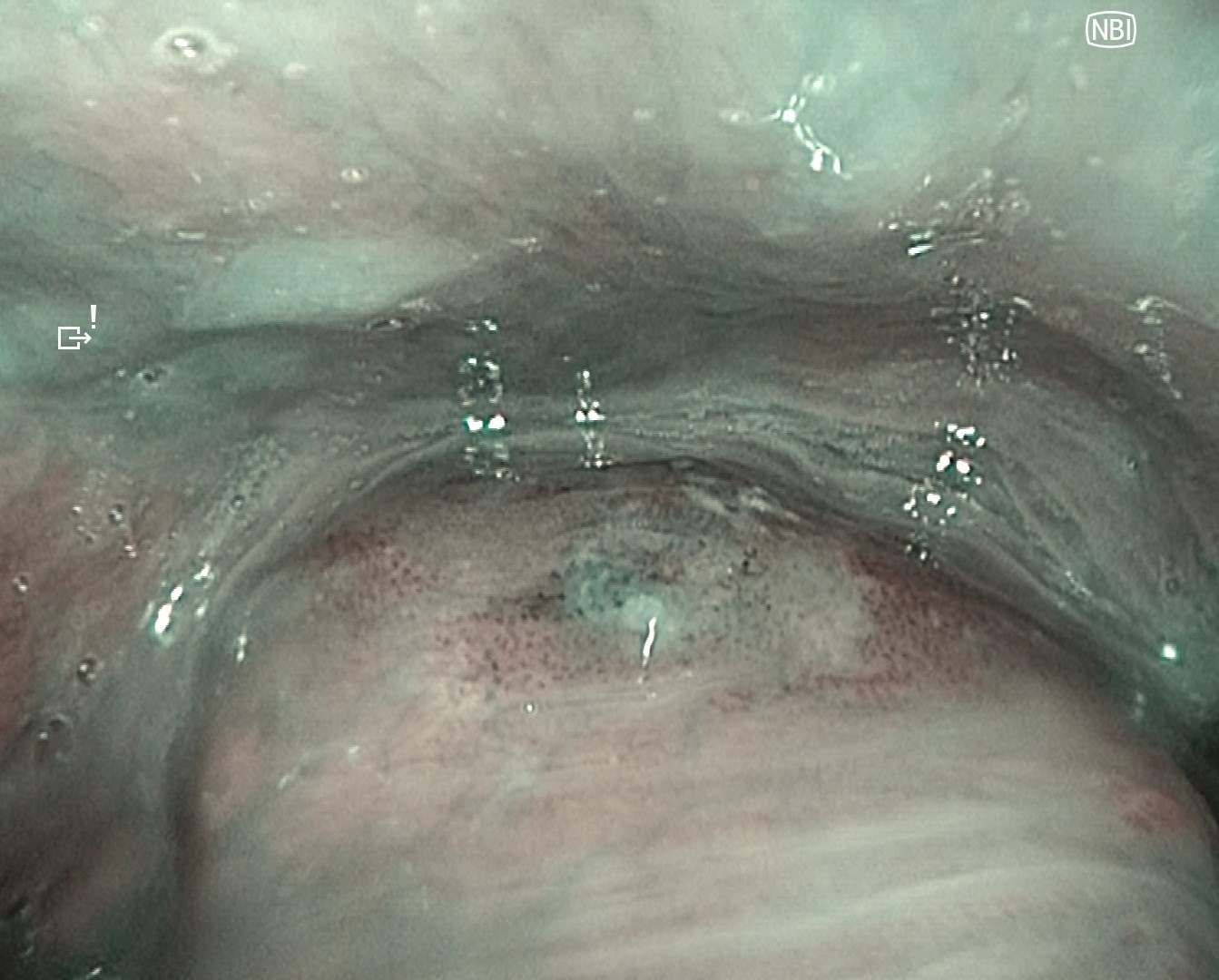
Under general anesthesia, the left pyriform sinus was observed after hypopharyngeal exposure. A well-defined brownish area with atypical microvessels was identified.
In my opinion, compared with the VISERA ELITE™ OTV-S190 system, the VISERA™ S OTV-S500 system supported visualization of lesion structure and surface characteristics in this case.
Representative NBI™ images obtained during clinical evaluation under comparable imaging conditions.
NBI™ Technology Image
Video System Center: VISERA ELITE™ OTV-S190 System
Video Rhinolaryngoscope: ENF-VH

NBI™ Technology Image
Video System Center: VISERA™ S OTV-S500 System
Video Rhinolaryngoscope: ENF-VH
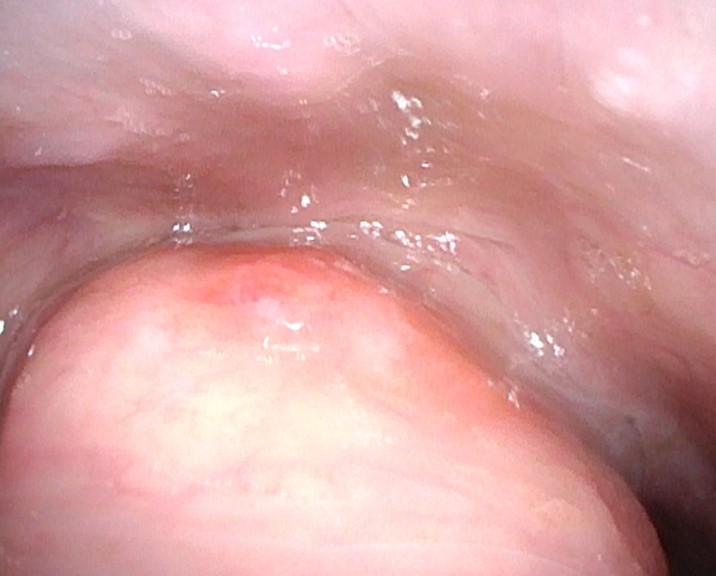
Case 4: Vocal Fold Carcinoma in Situ

A thin whitish lesion was observed on the vocal fold. No extension to the anterior commissure was noted, and NBI™ technology observation revealed no surrounding atypical vessels. Stroboscopic examination demonstrated relatively preserved mucosal wave motion, suggesting the absence of deep tissue invasion.
Case 5: Final pathology confirmed spindle cell squamous cell carcinoma of the Right Vocal Fold

Disclaimer: Representative clinical case shown for educational purposes. Clinical interpretation should be integrated with standard diagnostic evaluation.
During initial endoscopic assessment, a white, elevated lesion was observed on the right vocal fold. NBI™ technology observation revealed clustered vascular structures posterior to the white lesion; however, no surrounding brownish area or atypical vessels were observed, and no extension to the anterior commissure was identified. Stroboscopic examination showed reduced mucosal wave motion of the right vocal fold, raising clinical suspicion for malignant involvement pending comprehensive clinical and pathologic evaluation. During sustained phonation, supraglottic constriction was also observed.
Representative stroboscopic examination from a clinical case for educational visualization purposes.
Case 6: Left Vocal Fold Paralysis

Disclaimer: Representative clinical case shown for educational purposes. Individual procedural findings and outcomes may vary.
A patient with left vocal fold paralysis caused by esophageal cancer invasion underwent type I thyroplasty and arytenoid adduction under local anesthesia. Intraoperative stroboscopic observation was used to assess vocal fold medialization and mucosal vibration during the procedure. Intraoperative visualization supported assessment of mucosal vibration during surgical adjustment of medialization. In this representative case, maximum phonation time increased from 4.6 seconds to approximately 20 seconds following intraoperative adjustment.
Representative intraoperative stroboscopic visualization during clinical assessment.
Conclusion
In the light-source-integrated VISERA™ S OTV-S500 system, in my opinion, enhanced image processing performance may lead to improvements in imaging capability. In addition to conventional white-light observation, the system provides NBI™ technology and stroboscopic observation with sufficient illumination, both of which can be switched using a single operation. “These features may support lesion visualization during clinical assessment.
By appropriately utilizing the characteristics of this system, it may support clinical assessment and workflow efficiency, offering significant benefits for both patients and healthcare providers. The VISERA™ S OTV-S500 system supports clinical workflow across a range of head and neck applications and may support endoscopic visualization and clinical evaluation.
Disclaimer
The techniques and clinical opinions presented in this material reflect the personal experience and professional judgment of the healthcare professional and do not necessarily represent the views of Olympus. This material is intended for healthcare professionals only. This material is not intended to substitute the Instructions for Use (IFU). Users should always refer to the applicable IFU and use Olympus products in accordance with the approved indications and local regulatory requirements. The healthcare professional presenting this material has been engaged by Olympus and compensated at fair market value for their services.
- Content Type