Gastric Case 7

Dr. Kunihisa Uchita
Kochi Red Cross Hospital
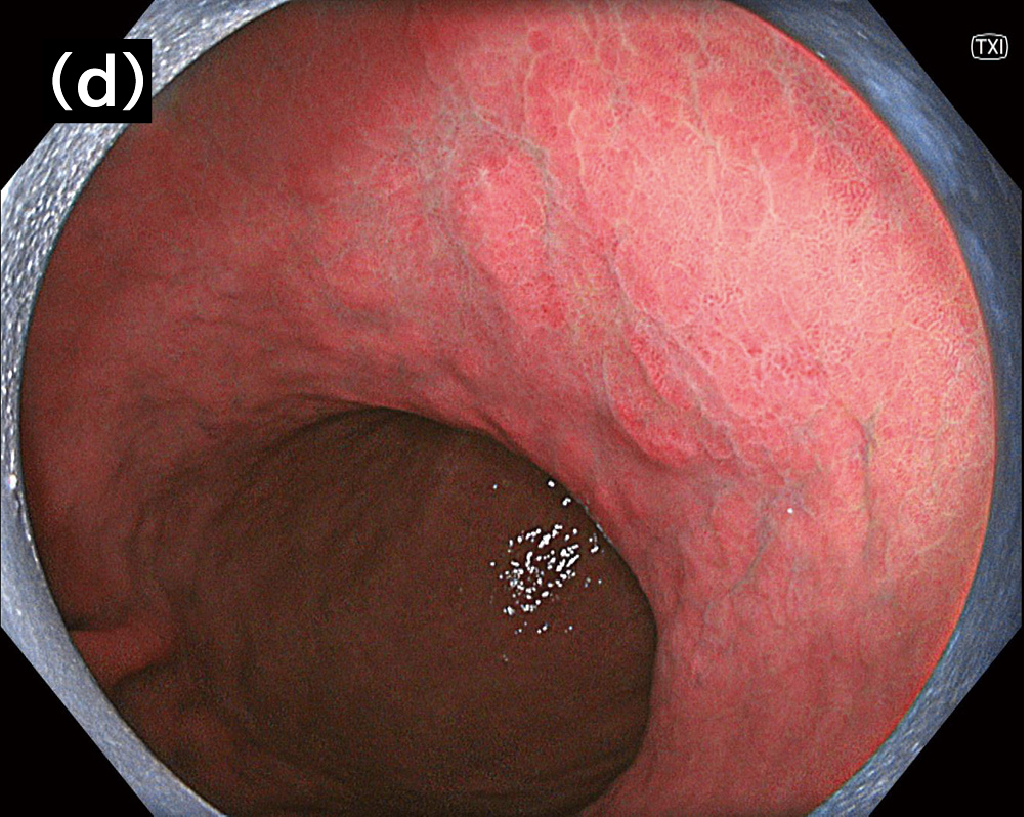
The XZ1200 effectively detects lesions in post- eradication cases with its improved visibility of slight changes in color and unevenness of the mucosa
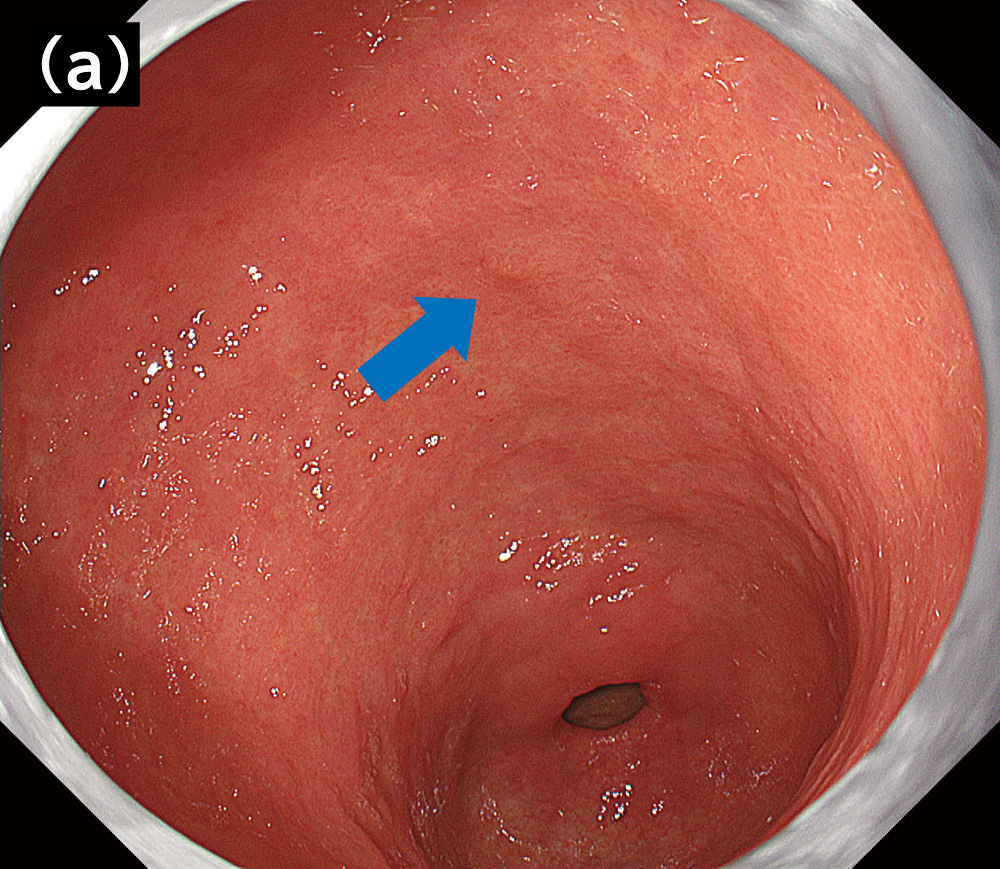
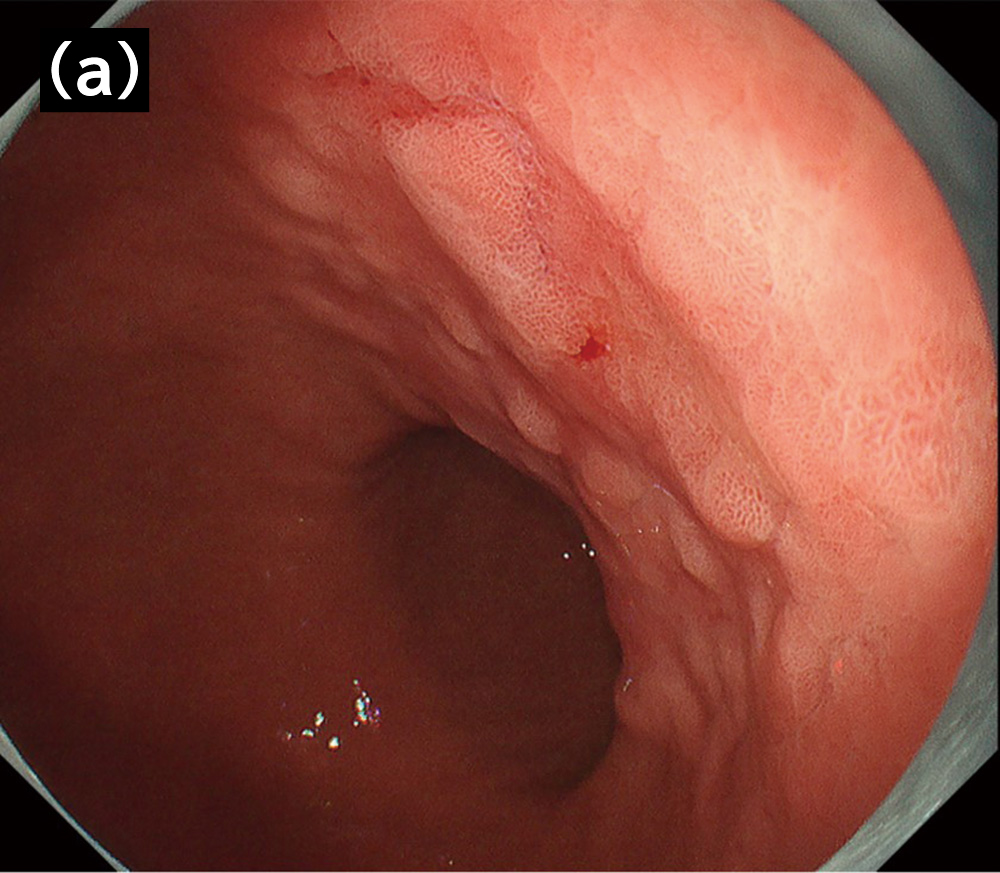
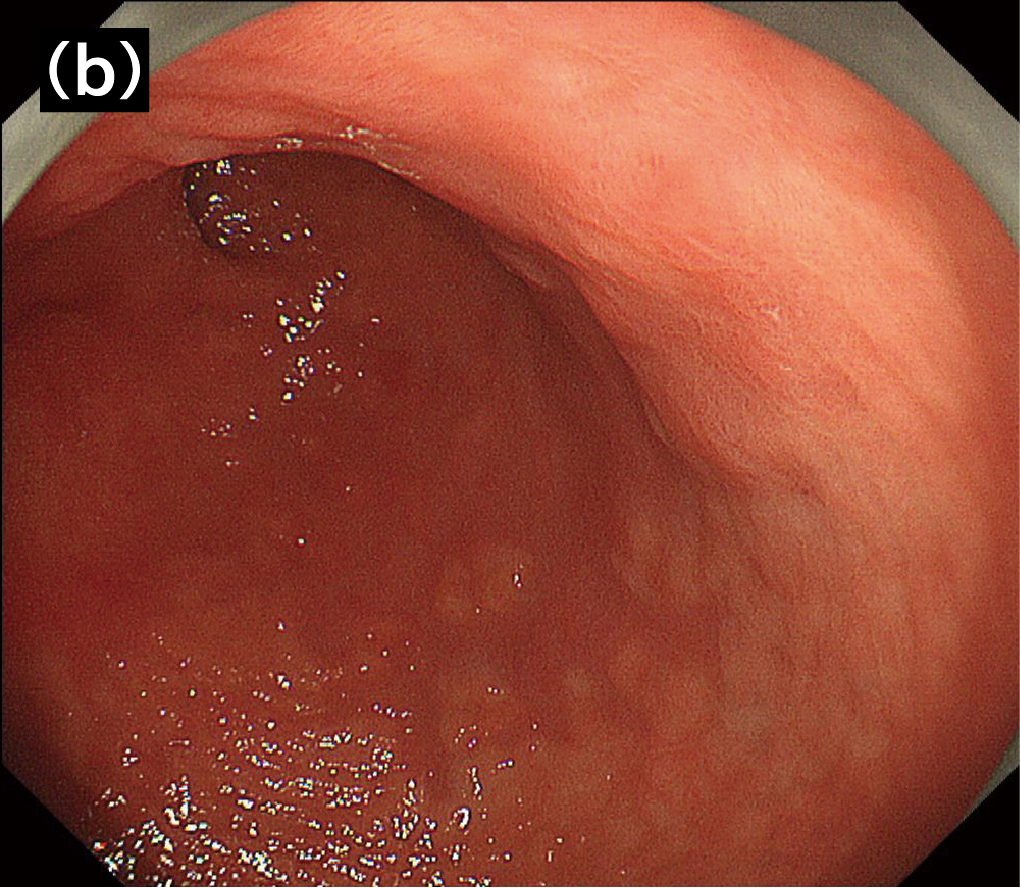
In recent years, post-eradication gastric cancer has been on the rise, with Helicobacter pylori eradication therapy becoming increasingly common. I find that the number of patients suffered from post-eradication gastric cancer is also increasing at our hospital (Kochi Red Cross Hospital). Because the appearance of both the background mucosa and the lesion itself is affected, their boundary is obscure in many cases of post-eradication cancer1) compared with
H. pylori-infected cases. The lesion detection of this type of cancer is sometimes said to be difficult.
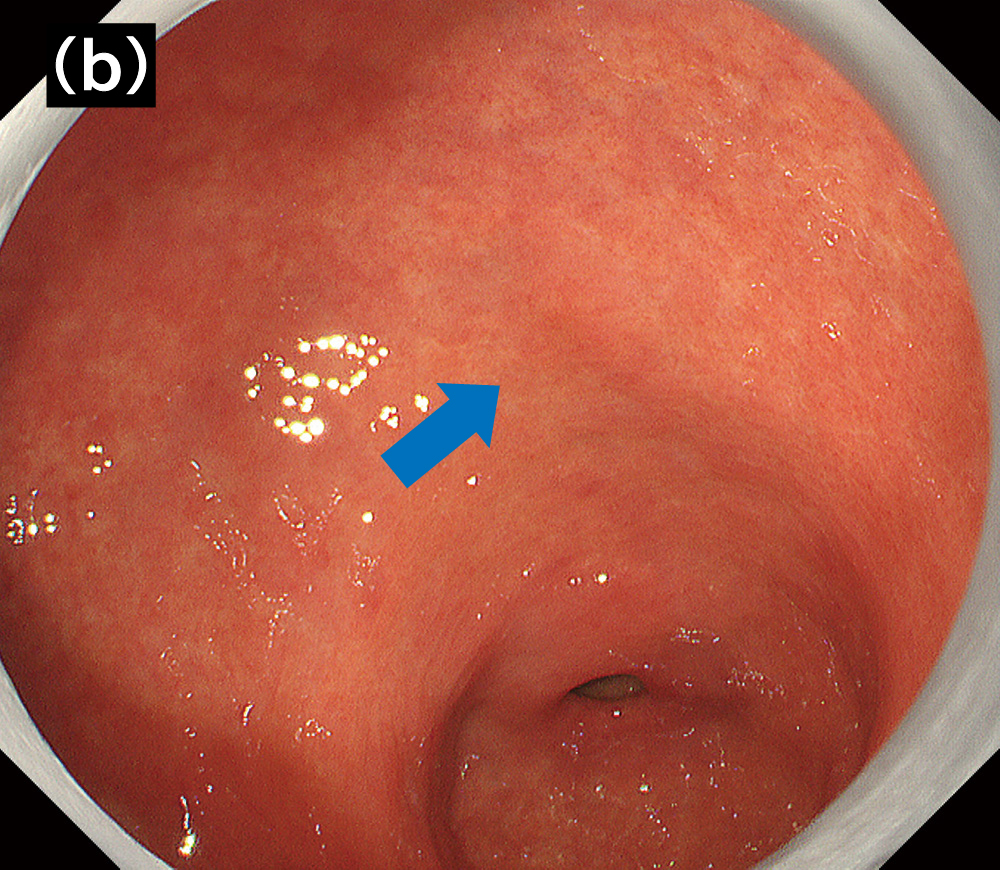
The newly released GIF-XZ1200 (hereafter XZ1200) shows less noise images compared with GIF-H290Z which has been conventionally used at our hospital for screening. XZ1200 also provides higher image quality than that in the previous high-definition models. Therefore, I find that the XZ1200 is especially useful in post-eradication cases in which the lesion detection is difficult. Although the differentiation of gastric cancer and atrophic gastritis in post-eradication cases can be difficult because of similar appearances of these lesions, I have an impression that the endoscopy with the XZ1200 makes this kind of differentiation easy. This is because the clear imaging of subtle changes in color and unevenness of the mucosa by using the XZ1200 can improve the visibility of the boundaries between the background mucosa and the lesion (Fig. 1).
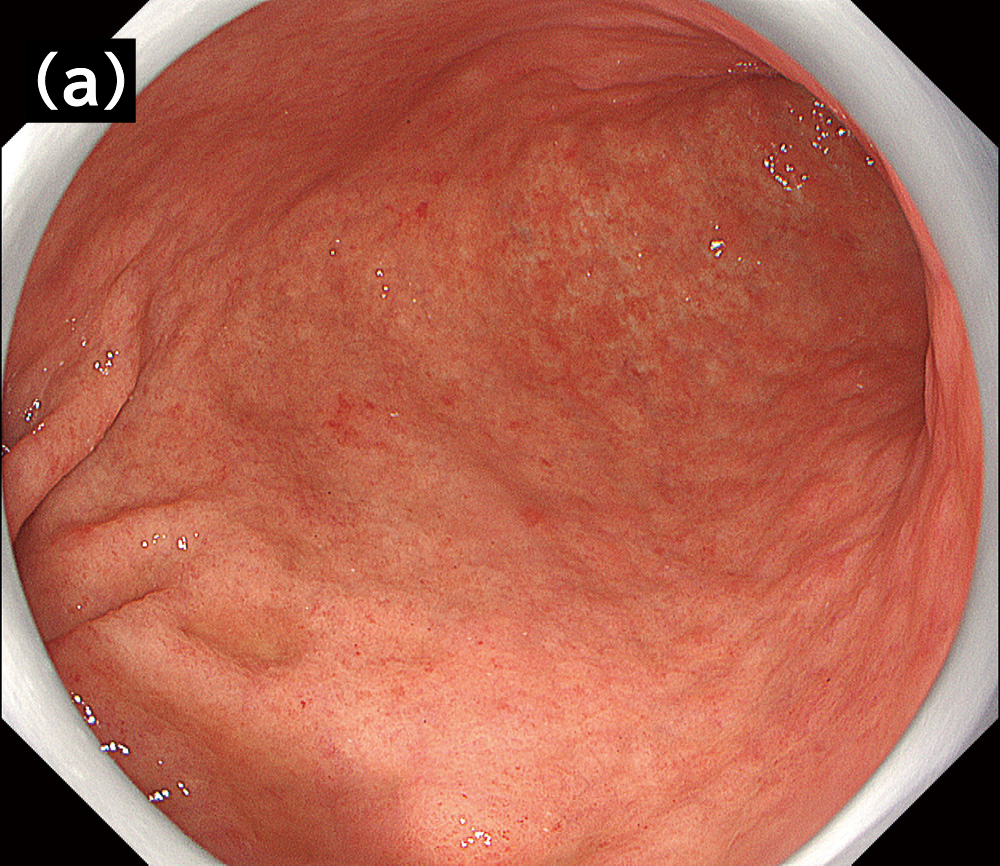
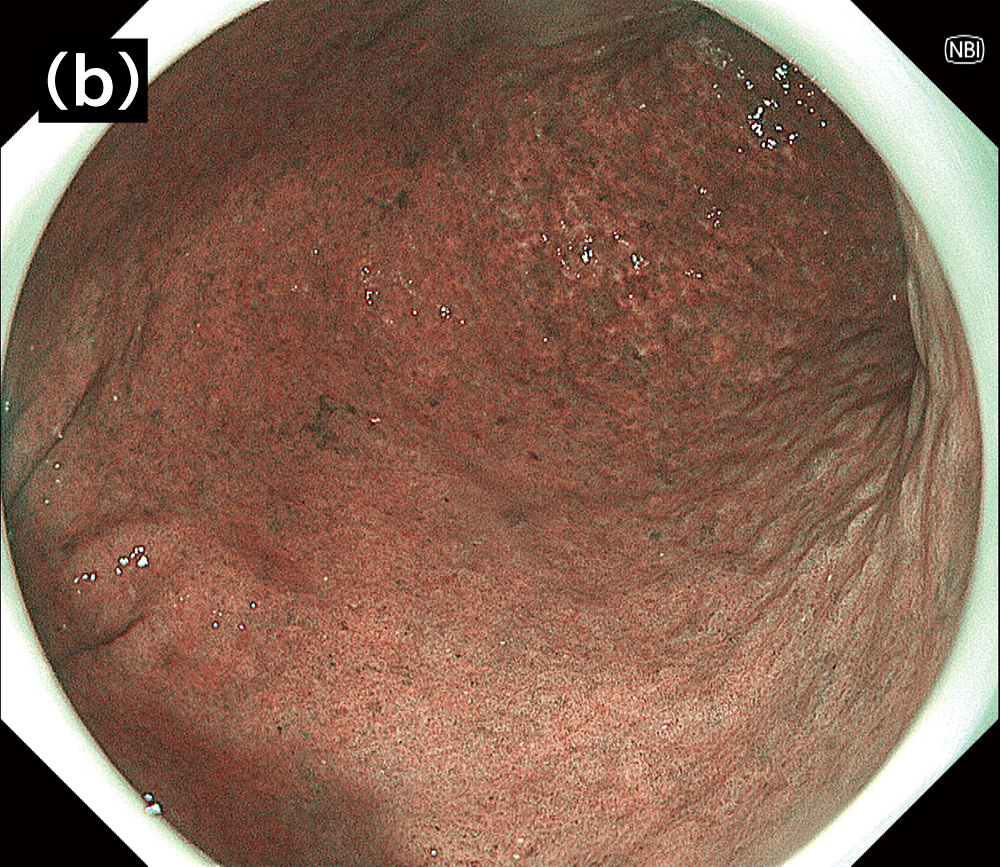
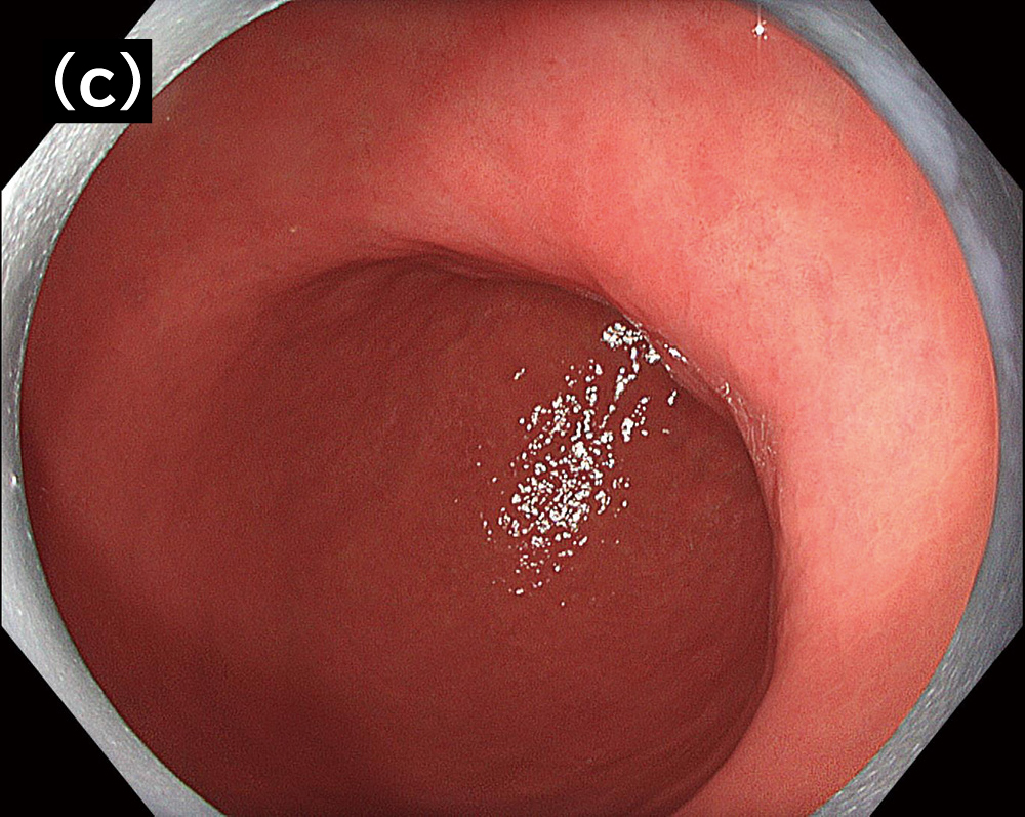
High image quality can be realized particularly in middle to long distance view under NBI. The monitor view is dark, and the images become noise-prone in this situation with conventional endoscopes. The XZ1200 enables capturing of brighter and clearer endoscopic images with less noise in middle to long distance view under NBI, which will be useful for lesion detection (Fig. 2). Besides, color misregistration appears to be reduced in the use of the XZ1200 adopted with a high- speed sequential-frame method*1. It will work even in areas frequently captured with color misregistration because of respiratory fluctuations and pulsation, which results in a smoother presentation of the endoscopic video image.
Mist removal is a key to taking clearer images using the XZ1200, as it enables high-resolution imaging without blurring
In conventional endoscopes with sequential-frame method, retakes of images were occasionally required because respiratory fluctuations and pulsation during imaging caused blurring and/or color misregistration. The generation of blurring and color misregistration has reduced thanks to the XZ1200 adopted with the high-speed sequential-frame method. I believe that the capturing efficiency of endoscopic images has improved by the decrease in the number of retakes in use of the XZ1200.
At our hospital, we use air delivery and suctioning at the same time to remove the mist generated from water irrigation and lens washing, and then supply air before capturing images for the acquisition of clearer images. This is because the mist floating in the lumen can appear in imaging area and cause color misregistration of endoscopic images taken with conventional sequential-frame method. However, due to its high-speed sequential- frame method, the XZ1200 reduces mist-caused color misregistration, which will enables the easy acquisition of clearer images.
The XZ1200 enables the confident evaluation of microvascular pattern with its maximum optical zoom of ×125
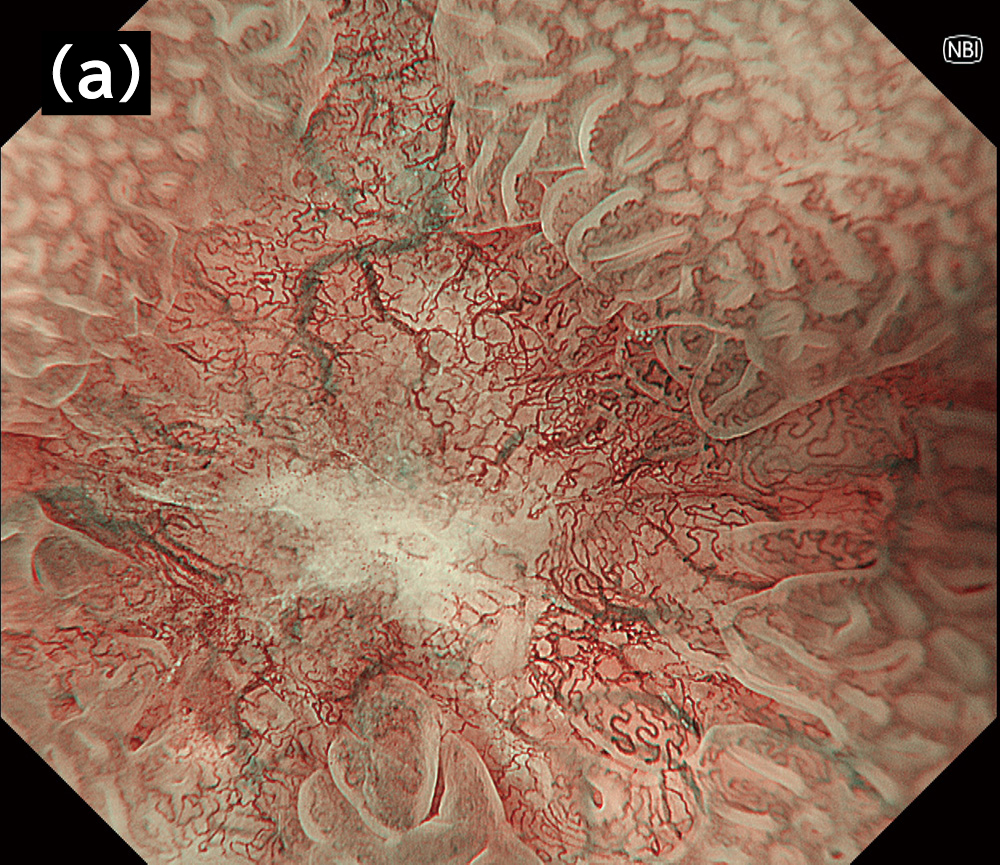
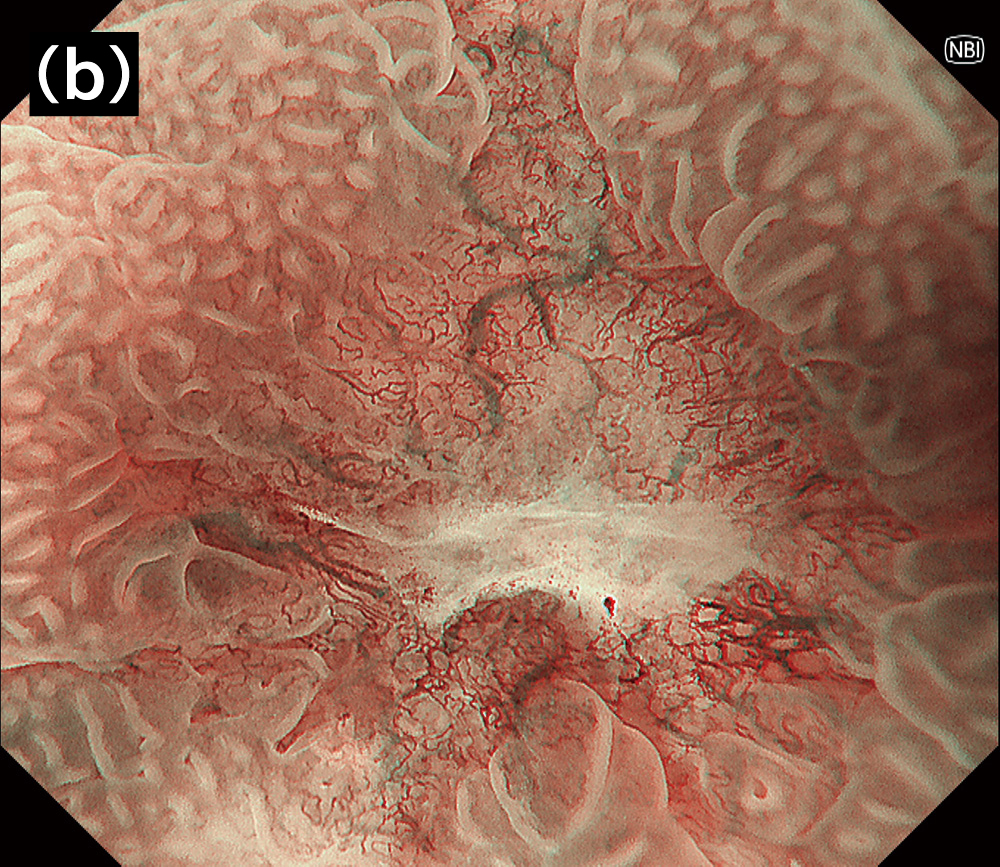
GIF-H260Z, with the maximum magnification of ×105*2, has been used at our hospital for thorough examinations. I find that the optical zoom function*3 in the XZ1200 with the maximum magnification of ×125 enables a detailed observation of capillaries — while maintaining high image quality — in magnifying endoscopic observation(Fig.3).Consequently, I have an impression that a more confident and quick evaluation of microvascular pattern has become possible for certain microlesions during the diagnosis of detected gastric lesions with the diagnostic system MESDA-G under magnifying endoscopy.
Particularly, in the case of post-eradication cancer of which qualitative and demarcation diagnosis are difficult as well as detection, we observe the lesion at the maximum magnification using an endoscope with a distal hood attached. When it is still difficult to diagnose, fine minute capillaries should be observed during pushing aside and unfolding the mucosa by the distal hood. In the conventional endoscopy, distal hoods make the monitor view darker. However, I find that the XZ1200 enables the sufficiently bright monitor view even with a distal hood, and detailed observation compared with previous models. Additionally, even when the optical zoom is combined with the electronic zoom function for the further magnification, high image quality appears to be maintained in the XZ1200 because of the prevented noise increase. I believe that the high image quality and high magnification of the XZ1200 may advance the efficiency of detailed examinations and the accuracy of qualitative diagnosis of detected gastric lesions during magnifying endoscopic observation.
*2: When CV-290 and OEV262H are combined *3: When CV-1500 and OEV321UH are combined
TXI and BAI-MAC incorporated in the EVIS X1 improve the efficiency and accuracy of not only screening tests, but also detailed examinations and endoscopic treatments (*used endoscopes: GIF-EZ1500 and GIF-H260Z)
The EVIS X1 is equipped with TXI, one of the image enhancement endoscopies. I find that TXI is effective in detection of the lesion which is difficult to be observed under white light imaging (WLI). This is because it enhances slight color difference of lesions with less color tone changes and subtle unevenness of flat lesions. At our hospital, observation under WLI is basically used for detection, and we switch to the TXI when it is difficult to judge. We utilize TXI as a modality to capture slight color differences and uneven surfaces to avoid overlooking lesions.
Previously, I have experienced ESD of a lesion which changed its morphology after its detection and became difficult to be observed on the day of ESD. At that time, I could successfully capture the demarcation of the lesion and performed ESD with the help of the enhancement of color and unevenness provided by TXI with GIF-EZ1500 (Fig. 4). With conventional endoscopes, identification of the detected lesions was difficult when the lesions changed their morphology after detection. I find that TXI enables quick identification of such lesions in detailed examinations and endoscopic treatments.
BAI-MAC incorporated into the EVIS X1 is always turned on during screening examinations at our hospital. In my experience, BAI- MAC enables better observations of near to far points in middle to long distance view by increasing the brightness of far points while maintaining the brightness of near points.
I believe that the functions of the EVIS X1 (such as TXI and BAI- MAC) advance the efficiency and the accuracy of screening tests. Furthermore, in detailed examinations and endoscopic treatments, they will also work effectively for the identification of lesions which has changed its morphology after the detection.
The XZ1200 is expected to improve the efficiency and the quality of endoscopic diagnosis and treatment, and endoscopists using the XZ1200 will be required to improve their skills
I believe that the advanced observation performance of the XZ1200 due to its high magnification, high resolution, and high- speed sequential-frame method imaging can be realized in various situations of endoscopic diagnosis (including screening tests and detailed examinations) by every endoscopist regardless of their experiences. However, observational/diagnostic skills may be required of endoscopists for detection and qualitative diagnosis with higher accuracy, as the XZ1200 captures minute changes in color/ unevenness of the mucosa during screening tests.
Further advance in the efficiency and the quality of endoscopic examinations/treatments will be achieved by a combination of the high observation performance of the XZ1200 and significant expertise of endoscopists.
References
1 Kiminori Ito, et al., Gastroenterological Endoscopy, 2018, Volume 60, No. 1, pp. 5-13
- Keyword
- Content Type