Pancreatobiliary case 3

Jong Ho Moon, MD, PhD, FASGE, FACG, FJGES
Professor of Medicine
Director, Digestive Disease Center
SoonChunHyang University School of Medicine,
Bucheon/Seoul, Korea

Il Sang Shin, MD, PhD
Assistant Professor
Digestive Disease Center
SoonChunHyang University School of Medicine,
Bucheon/Seoul, Korea
Disclaimer:
- NBI™, RDI™ and TXI™ technologies are not intended to replace histopathological sampling as a means of diagnosis
- NBI™, RDI™, and TXI™ technologies are 510(k) cleared in the United States. This case study is being furnished to provide examples of NBI™, RDI™, and TXI™ technology use. The TJF-Q290V used in this case is not available in the US market at this time, nor is there an established time for its release. The safety and effectiveness of this product and/or the use of these products has not yet been established in the United States market.
- The positions and statements made herein by Dr. Moon and Dr. Shin are based on their respective experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
1 ) Data on file with Olympus (DC00489968)
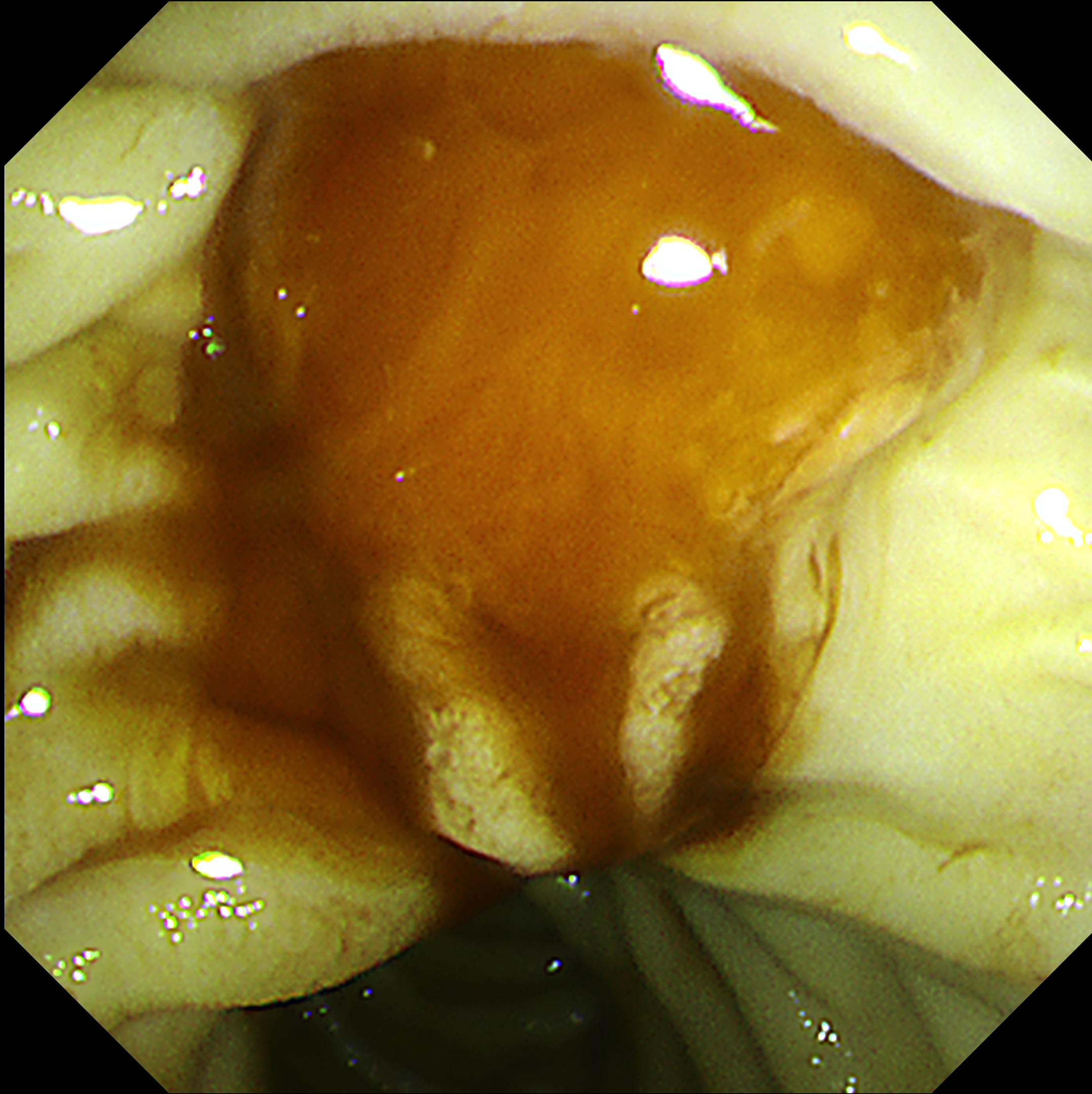
Scope: TJF-Q290V
Organ: Ampulla of Vater
Patient information: F, 50s
Medical history: None
1. WLI Observation

Enhancement : A7
NBI Mode : NA
TXI Mode : NA
RDI Mode : NA
BAI-MAC : On
2. NBI™ technology Observation
Enhancement : A7
NBI Color Mode : 2
TXI Mode : NA
RDI Mode : NA
BAI-MAC : On
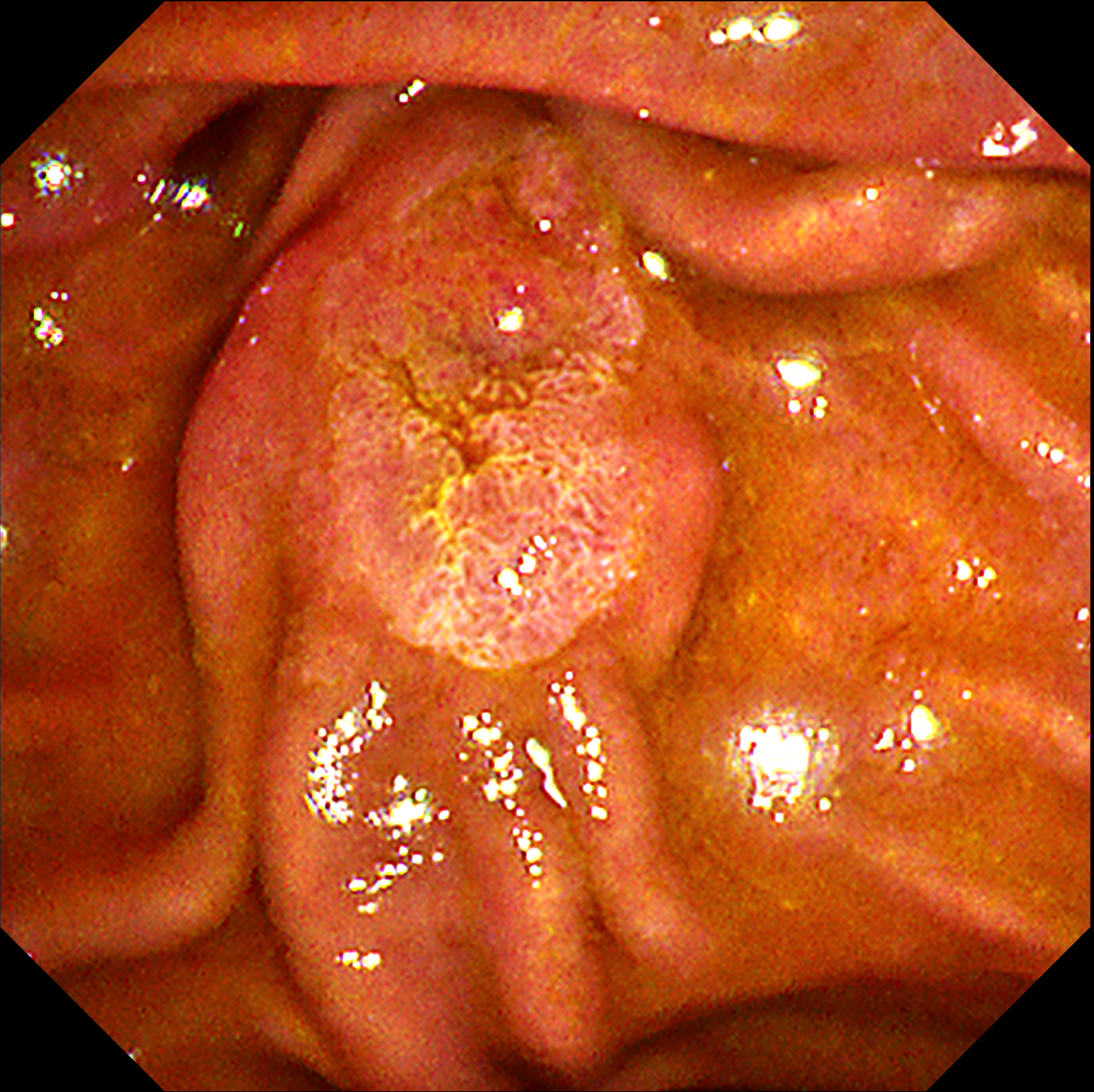
3. TXI™ technology Observation

Enhancement : A7
NBI Mode : NA
TXI Mode : 1
RDI Mode : NA
BAI-MAC : NA
4. TXI™ technology Observation
Enhancement : A7
NBI Mode : NA
TXI Mode : 2
RDI Mode : NA
BAI-MAC : On
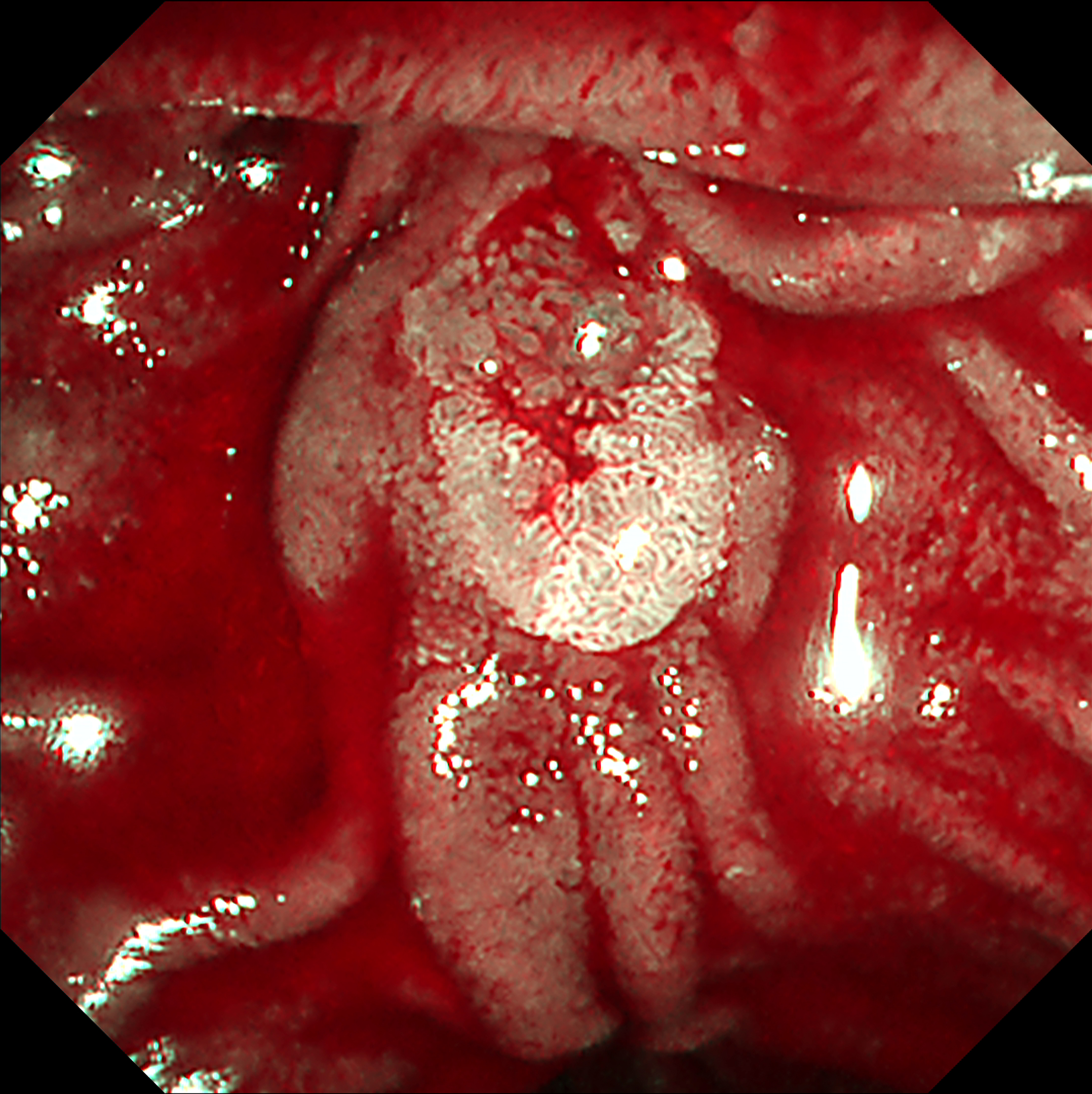
5. RDI™ technology Observation

Enhancement : A7
NBI Mode : NA
TXI Mode : NA
RDI Mode : 3
BAI-MAC : NA
6. NBI™ technology observation
Enhancement : A7
NBI Color Mode : 2
TXI Mode : NA
RDI Mode : NA
BAI-MAC : On
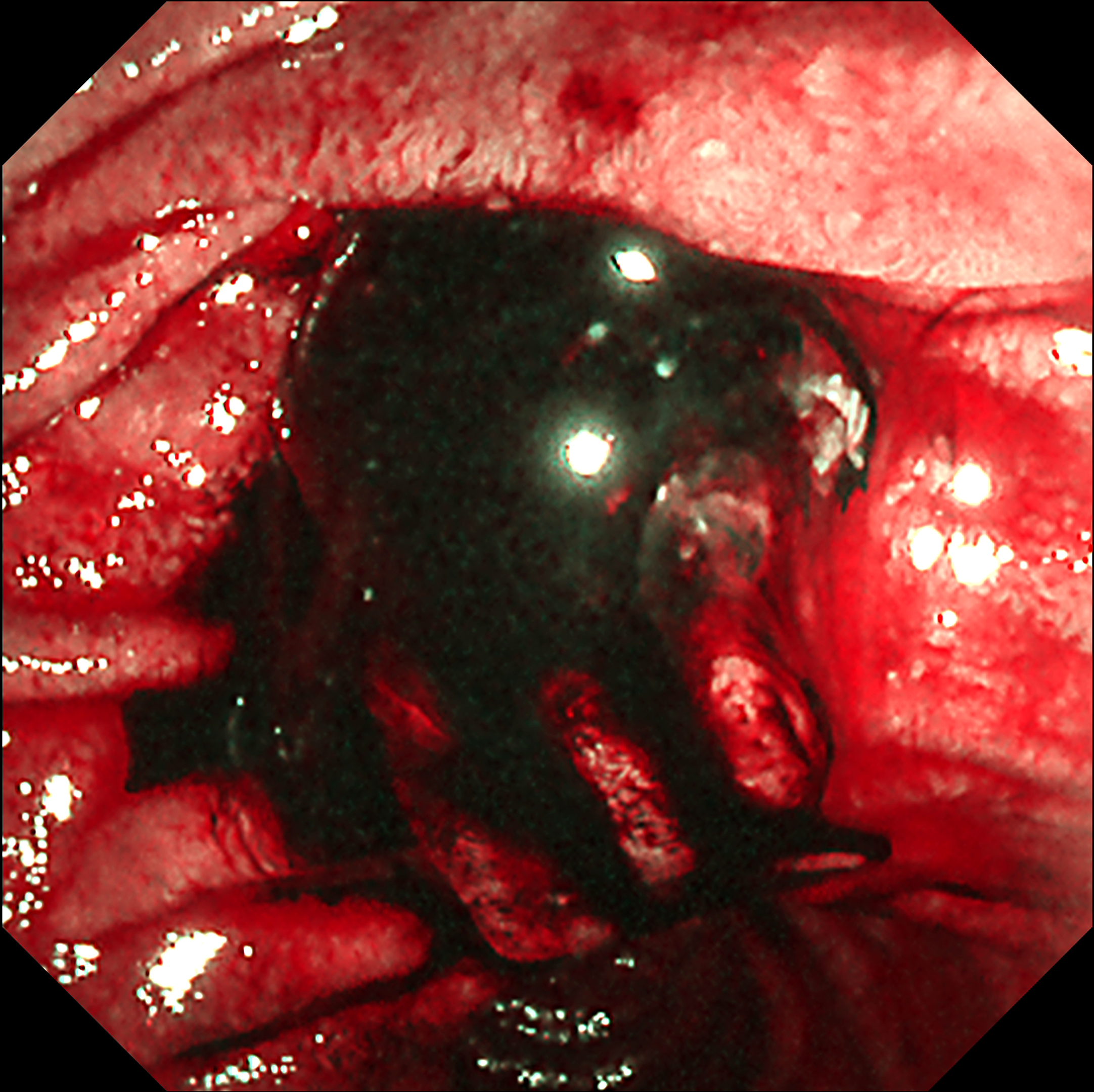
7. RDI™ technology Treatment
Enhancement : A7
NBI Mode : NA
TXI Mode : NA
RDI Mode : 1
BAI-MAC : On
Case Video
This video demonstrates the utility of an image enhanced endoscopy system in identifying bile acid-rich ampullary lesion. A well-defined ampullary lesion was observed in white-light imaging (WLI), but detailed observation was difficult in narrow-band imaging (NBI™) observation mode due to the interference from bile acid. TXI™ technology modes provided more information of surface structural features including hyperemic microvasculature beneath circular fold with less interference from bile acid1. RDI™ technology mode 3 provided detailed information of ampullary lesion for targeted forceps biopsy without any interference from bile acid. After forceps biopsy, RDI™ technology mode 1 could easily identify the hemostatic status of the ampulla of Vater, making it easy to determine whether there are bleeding points requiring endoscopic hemostasis compared to NBI™ technology. When detailed observation using NBI™ technology is difficult due to bile acid, applying TXI™ and RDI™ technologies can be helpful for evaluation of abnormalities of ampulla of Vater.
DISCLAIMER:Information regarding competitor products is presented to the best of our knowledge as of the date of presentation. This material does not constitute medical or legal advice and should not be relied upon as such. It should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, warnings and cautions. Techniques, instruments and setting can vary from facility to facility, and it is the clinician’s decision and responsibility in each clinical situation to decide which mode and settings to use.
Overall Comment
This case suggests that observation using TXI™ and RDI™ technology modes can be useful for the evaluation of suspicious adenomatous lesion of ampulla of Vater. TXI™ observation mode can be less disturbed by bile acid than NBI ™ observation and enhanced accurate evaluation of the ampullary lesion including hyperemic microvasculature beneath covering fold by emphasizing color differences of the mucosal surface. RDI™ technology mode 3 is not disturbed by bile acids at all, enabling accurate assessment of ampullary lesions and guiding the location for targeted forceps biopsy. Compared to NBI™ technology or white light, RDI™ technology mode 1 can effectively identify hemostatic status and potential bleeding points1.
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer
- Content Type