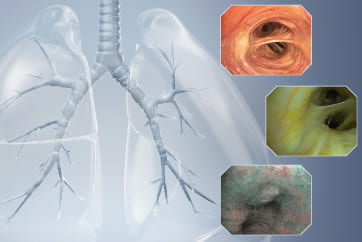
Case: Neoplasm in the right upper lobe bronchu

Professor Wang Guangfa, Guidance Expert
Chairman of the Department of Respiratory Diseases & Department of Respiratory and Critical Care Medicine,
Peking University First Hospital
Disclaimer:
- TXI™ and RDI™ Technologies are not intended to replace histopathological sampling as a means of diagnosis
- The positions and statements made herein by Dr. Guangfa, are based on Dr. Guangfa’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- The BF-1TQ290 used in this case is not available in the US market at this time nor is there an established time for its release. The safety and effectiveness of this product and or the use of these products has not yet been established in the United States market.
- The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
- Dr. Guangfa the authoring physician of this presentation, is a paid consultant to Olympus Corporation
Scope: BF-1TQ290
Case: Right upper lobe bronchus
Patient information: 74 years old, Male
Medical history: The patient developed cough with some white sputum for 2 weeks, without fever, hemoptysis, chest pain and other symptoms. Bronchoscopy showed “neoplasm in the right upper bronchus” and biopsy showed “bronchial mucosa and necrotic tissue”. Antibiotics and mucolytics were given. The patient had smoked 2 packs a day for 40 years and had quit smoking for 2 years.
1. In WLI, the neoplasm in the right upper bronchus blocked the lumen completely. A tumor protruded into right main bronchus from its orifice.
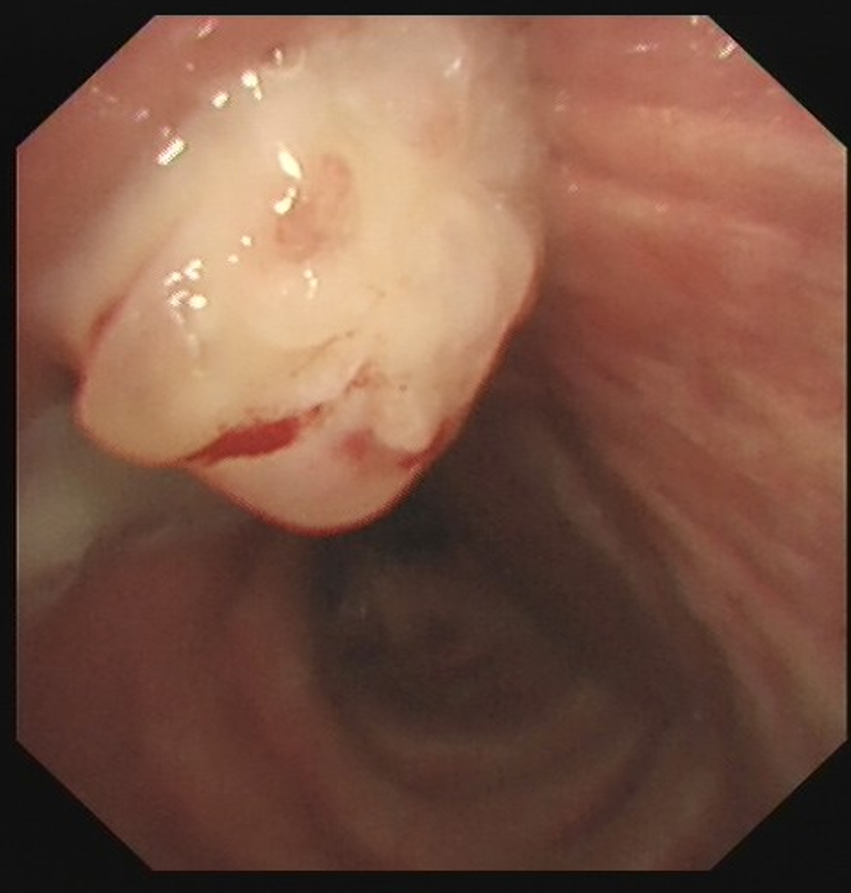
The surface details of the neoplasm were not clearly displayed in WLI mode. Thus, it was impossible to differentiate necrotic tissue from submucosal blood vessels.
2. In TXI™ technology mode 2, the three-dimensional structure of the neoplasm was clearer, and the details of the mucosa were revealed very well.
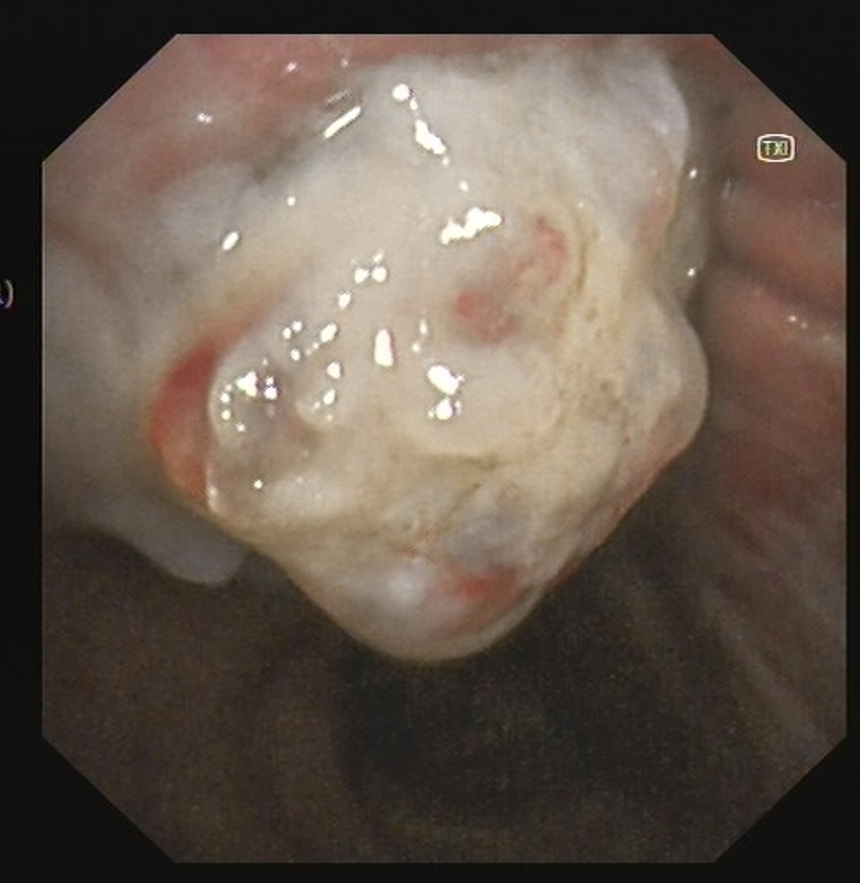
TXI™ technology mode 2 could reveal the subtle structures. The tones difference of the submucosal membrane was enhanced, and clearer observation was allowed.
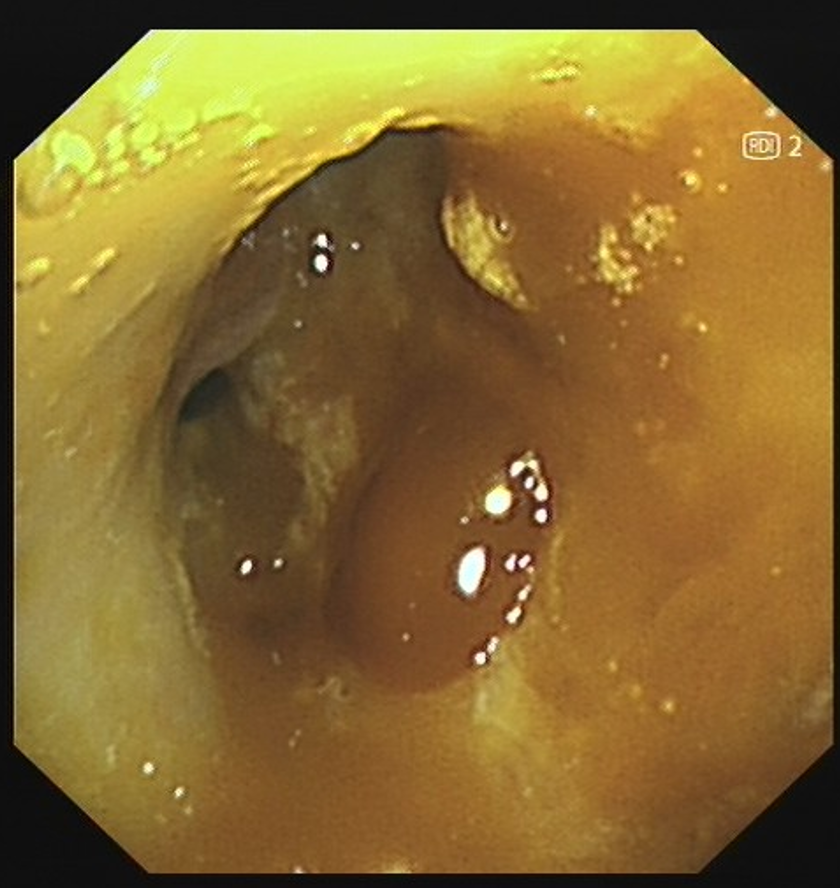
3. In RDI™ technology mode 2, submucosal blood vessels of the neoplasm were not observed

The RDI™ technology mode 2 can be used to observe deep blood vessels more clearly and assist in identifying whether there is any blood vessel at the biopsy site. Thereby the operator can avoid biopsies at the site with rich blood vessels and reduce the risk of bleeding.
4. Active bleeding was seen in WLI mode after the resection of neoplasm

Novices tend to be flustered when facing bleeding. Poor visibility of the exact bleeding point will influence the judgement and hemostatic efficiency. The bronchoscopy procedures will be delayed.
5. After resection of the neoplasm, the RDI™ technology mode 1 filtered out the red interference of blood, making it easier to determine the bleeding site
The RDI™ technology Mode 1 improves the visibility of bleeding points, facilitates rapid hemostasis, and potentially reduces operator stress caused by bleeding
Overall comment
The TXI™ technology (optical function) and RDI™ technology of the bronchoscope help distinguish the fine structure of the bronchial mucosa, improve the visibility of bleeding points, help stop bleeding quickly, and improve the efficiency and safety of endoscopic diagnosis and treatment.
Co-operator:
Professor Wang Xi, Operation Expert
Associate Chief Physician, Department of Respiratory and Critical Care Medicine,
Peking University First Hospital
- Content Type