Case: Thermal Ablation of Adenoid Cystic Carcinoma of the Left Main Bronchus
Director Bai Chong
Department of Respiratory and Critical Care Medicine,
the First Affiliated Hospital of Naval Military Medical University
(Shanghai Changhai Hospital)
Deputy Director, Huang Haidong
Department of Respiratory and Critical Care Medicine,
the First Affiliated Hospital of Naval Military Medical University
(Shanghai Changhai Hospital)
Professor Shi Dongchen
Department of Respiratory and Critical Care Medicine,
the First Affiliated Hospital of Naval Military Medical University
(Shanghai Changhai Hospital)
Disclaimer:
- RDI™ Technology is not intended to replace histopathological sampling as a means of diagnosis
- The positions and statements made herein by Dr. Chong, Dr. Haidong, and Dr. Dongchen are based on their experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- RDI™ technology is 510(k) cleared in the United States. The case study is being furnished to provide an example of this technology use. The BF-Q290 used in this case is not available in the US market at this time nor is there an established time for its release. The safety and effectiveness of this product and or the use of these products has not yet been established in the United States market.
- The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
- Dr. Chong, Dr. Haidong, and Dr. Dongchen, the authoring physicians of this presentation, are paid consultants to Olympus Corporation
Scope: BF-Q290
Case: Left main bronchus
Patient information: 56 years old, Female
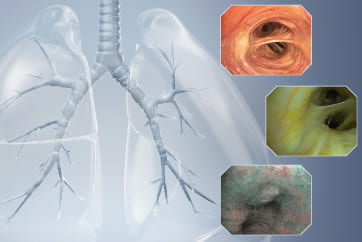
Medical history: The patient was diagnosed with adenoid cystic carcinoma of the left main bronchus with neoplastic stenosis for more than 10 years. After comprehensive treatment including placement of uncovered metallic stent in the left main bronchus, brachytherapy and radioactive seeds implantation for mediastinal lesions, her condition was stable. The patient had shortness of breath after activity in the past 2 weeks. Chest CT and bronchoscopy showed that tumor tissue growth in the left main bronchus stent had caused restenosis of the left main bronchus.
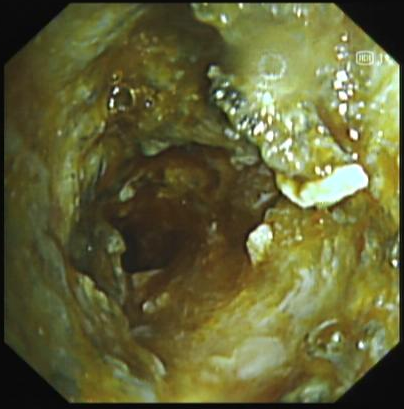
1. The opening of left main bronchus in WLI mode before thermal ablation treatment

Tumor tissue was observed growing inside the uncovered metal stent in the left main bronchus lumen and blocking the lumen.
2. Electrocoagulation for high-frequency thermal ablation is being performed on the tumor tissue in the left main stent in RDI™ technology mode
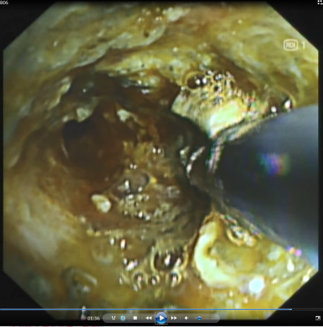
The thermal ablation field of view in RDI mode is clearer than that in WLI mode, which improves the efficiency and safety of thermal ablation.
3. After thermal ablation and recanalization, the lower trachea observed in RDI™ technology mode showed recanalization of the left main bronchus

The field of view was clear in RDI™ technology mode.
4. The lower trachea observed in WLI mode showed recanalization of the left main bronchus after thermal ablation and recanalization
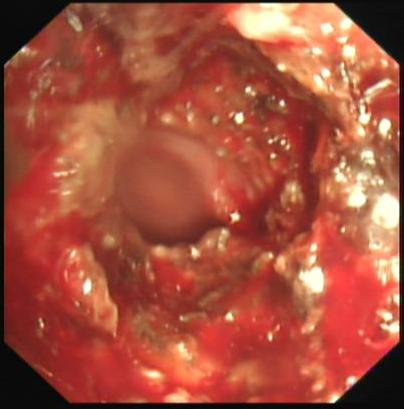
The tumor tissue invaded the stent in the lower trachea of the left main bronchus. After treatment, the lumen was more unobstructed than before. The tumor tissue was rich in capillaries and easily bled upon touch.
5. (The left main bronchus lumen was successfully recanalized after thermal ablation of the tumor in the metal stent lumen of the left main bronchus) RDI™ technology mode
The field of view was clear in RDI™ technology mode.
6. Endoscopic video
Endoscopy revealed that tumor tissue had invaded and blocked the lumen of the uncovered metal stent of the left main bronchus. The tumor tissue within the stent was rich in capillaries and easily bled upon touch. High-frequency electrocoagulation was given in RDI™ technology mode to repeatedly cauterize and ablate the tumor tissue. During the operation, the field of view was clear. After treatment, the lumen of the left main bronchus became more unobstructed.
Overall comment
Intraluminal thermal ablation of tracheal adenoid cystic carcinoma can effectively solve the problem of restenosis after stent placement. However, due to the abnormally rich capillaries in tumor tissue, the continuous bleeding of the bronchial mucosa caused by thermal ablation interferes with the field of view in WLI mode, affecting the accuracy and safety of the treatment and reducing the treatment efficiency. The RDI™ technology mode can effectively reduce the interference on the field of view caused by local bleeding, thereby improving the operational accuracy, efficiency and safety of thermal treatment and effectively avoiding thermal damage to normal mucosal tissue.
- Content Type