PLASMA Vaporization Procedure Steps
01|Cystoscopy with Inspection of Urethra
Inspection of the urethra and bladder.
Inspect left and right ostium, bladder, verumontanum, and internal and external sphincter.
Bladder tumors should be excluded.
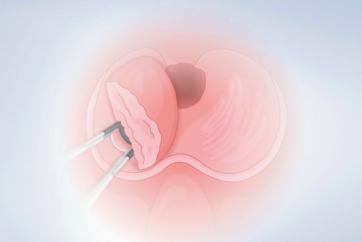
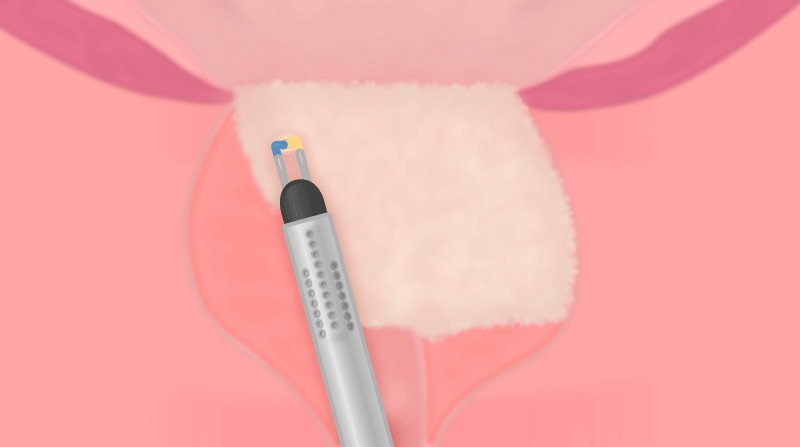
02|Marking of Resection Borders
Marking proximally of the verumontanum in the case of EP procedure.
Use the coagulation mode of the button to superficially mark the resection borders approximately two loop diameters proximally of the verumontanum.
If the area around the verumontanum is spared, postoperative retrograde ejaculation can be avoided. Whether this procedure also works with the vaporization technique remains unclear. There is a lack of research on this issue.
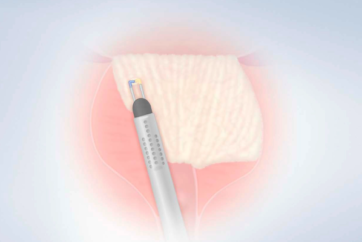
03|Vaporization of the Medial Lobe, of Basal Portions of Lateral Lobes, and of the Floor of the Prostatic Cavity
Vaporization of medial lobe and proximal part of the side lobes until the 5 o’clock and 7 o’clock position.


If bleeders occur do a spot coagulation without moving the button forwards and backwards (as known in monopolar surgery). To improve coagulation, use the edge of the button. If it is necessary to cut, use the edge of the button with vaporization mode.
04|Further Ablation of the Endovesical Part of the Medial and of the Left Lateral Lobe

05|Complete Vaporization of the Endourethral Part of the Left Lobe Except for an Apical Remnant

The vaporization direction goes from dorsal to ventral and the other way round until the left lobe is completely vaporized. Remove the tissue in layers in a vertical direction by starting on the floor of the cavity.
In most cases vessels are in the 11 and 1 o’clock position. Be aware of bleeders and do spot coagulation where needed.
PLASMA VAPORIZATION PROCEDURE STEPS
06|Ablation of the Endovesical Part of the Right Lateral Lobe
07|Complete Vaporization of the Endourethral Part of the Right Lobe Except for an Apical Remnant

The vaporization direction goes from dorsal to ventral and the other way round until the right lobe is completely vaporized. Remove the tissue in layers in a vertical direction by starting on the floor of the cavity.
08|Final Vaporization of the Apical Part
To avoid postoperative voiding disturbances, the BPH should be removed completely. At the apex remaining material can be vaporized or resected conventionally.

In contrast to the classical Barnes resection, all BPH material should be removed, also distal of the verumontanum.
09| Ensure Secure Hemostasis
Note
Ensure warm saline is used (37°C).
Be aware of bleeding and do spot coagulation where needed. Place the loop with slight pressure on the bleeding, activate coagulation mode and hold until bleeding has stopped.
The Nesbit Technique
Transurethral vaporization of the prostate can also be performed with the Nesbit technique. The method of Nesbit is aimed at a primary interruption of the arterial blood supply to the prostate adenoma. By encircling the adenoma tissue with a trench cut close to the capsule, all arteries supplying hyperplastic tissue are interrupted. The avascular prostatic tissue can then be excised rapidly with minimal blood loss.
- Keyword
- Content Type