Hiroshi Kawakami, MD, PhD
Professor and Chairman, Division of Gastroenterology and Hepatology, Department of Internal Medicine, Faculty of Medicine, University of Miyazaki
Academic/professional background:
1996 March Graduated from Graduate School of Medicine, Kitasato University
2005 March Completed Ph.D. course at Department of Gastroenterology and Hematology, Internal Medicine, Hokkaido University Graduate School of Medicine
2005 April Assistant Professor, Department of Gastroenterology and Hematology, Internal Medicine, Hokkaido University Graduate School of Medicine
2007 April Assistant Professor, Department of Gastroenterology and Hepatology, Hokkaido University Hospital
2015 October Lecturer and Clinical Associate Professor, Department of Gastroenterology and Hepatology, Hokkaido University Hospital
2016 April Professor and Chairman, Division of Gastroenterology and Hepatology, Department of Internal Medicine, Faculty of Medicine, University of Miyazaki
Case 1 Common bile duct stone case scheduled for endoscopic sphincterotomy (EST)
Procedure
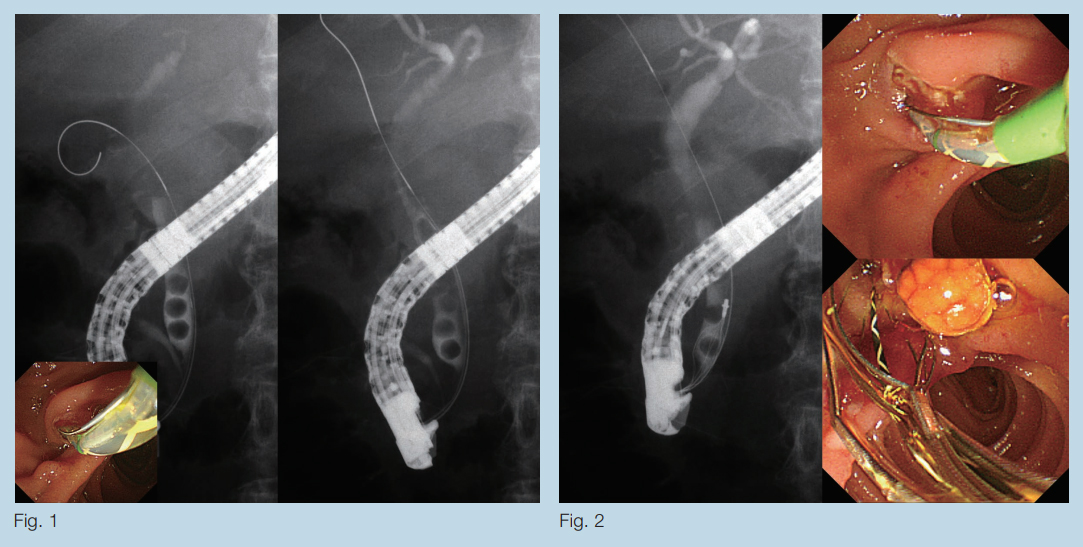
Selective biliary cannulation was performed by means of wire-guided cannulation (WGC) using the new CleverCut3V which features a short bending design. Subsequent cholangiography near the duodenal papilla confirmed the presence of several common bile duct stones (Fig. 1). We then moved the guidewire tip from the cystic duct into the intrahepatic bile duct (Fig. 1). Smooth guidance was possible through the short wire-compatible channel and complete stone removal was achieved (Fig. 2).
Case 2 Common bile duct stone case scheduled for EST
Procedure
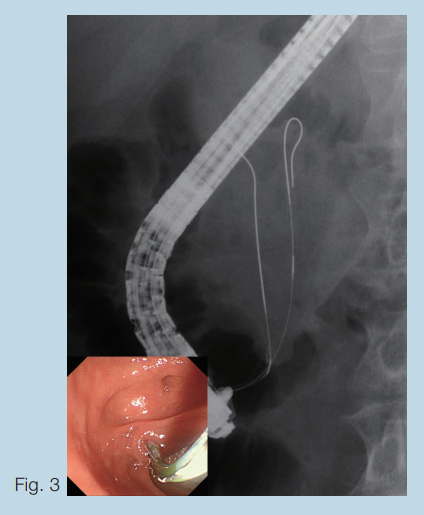
As with Case 1, we performed selective biliary cannulation by means of WGC. Remote operation was required because the major duodenal papilla was located near the horizontal limb. As accidental pancreatic duct insertion occurred, we immediately tried cannulation using the pancreatic guidewire technique. When we operated the device to point the distal end of the knife upward, we were able to reliably control the catheter and guidewire even with a sharp cannulation angle thanks to precise manipulation capability without projecting the catheter excessively from the forceps port (Fig. 3).
Discussion
In cooperation with Olympus Corporation, we have recently developed a novel, short-bending type CleverCut3V. Written below is the development background and the features of this product.
Selective biliary cannulation is essential to ERCP. In 1969, Japanese researchers Takagi et al.1 introduced cholangiography, and shortly afterwards Soma and Kawai et al. reported on EST 2, which was the precursor for a variety of therapeutic techniques. Selective biliary cannulation and EST remain the main techniques used in pancreaticobiliary endoscopy and various therapeutic devices have been developed for use in these procedures.
In Japan, cholangiography using an ERCP catheter with contrast medium injection is the core procedure in selective biliary cannulation. By contrast, in Europe and North America, wire-guided cannulation (WGC) is more commonly used. In WGC, biliary cannulation is performed by advancing a guidewire as if it is a tapered-tip catheter, rather than injecting contrast medium. In Japan, this technique has been widely spread since the early 2000’s. As it requires less time for selective biliary cannulation and x-ray exposure 3, this technique soon become the first choice.
In Japan, an ERCP catheter is mainly used for WGC, whereas in Europe and North America, the EST knives are used. Use of the ERCP catheters in Japan is based on the consideration that the catheter diameter and tip are thinner compared to the EST knives. There is also a cost problem when using multiple catheters. For another thing, in Europe and North America, a different type of duodenoscope is used than in Japan, which features a different backward oblique viewing angle 4. Therefore, selective biliary cannulation could be achieved more easily by bending the distal of the EST knife upward.
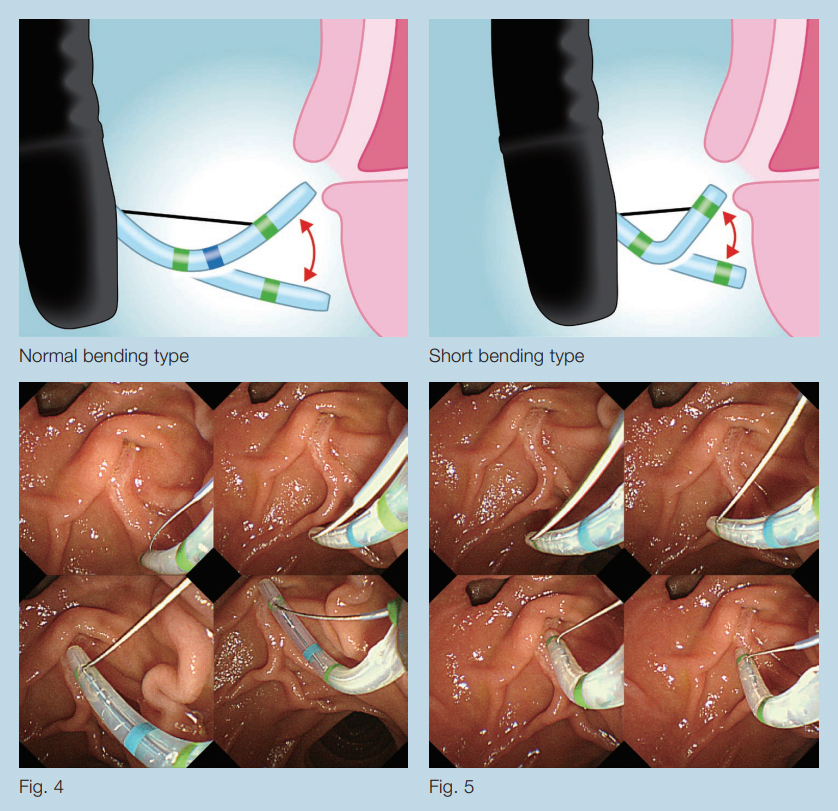
To deal with these problems, we developed a novel CleverCut3V with a short-bending design specifically for use as a cannulation knife in WGC 5. This new product inherits the triple lumen design and insulation coating (CleverCut coating) of the original CleverCut3 knife. New features include a more tapered distal end a short bending knife design to ensure short wire compatibility. When compared to the conventional product (Fig. 4), the shortening of the knife’s bending radius makes it easier to control, allowing the knife to bend without projecting it as far from the forceps port (Fig. 5). In addition, more stable imaging is possible than with an ERCP catheter, making possible more detailed evaluation of the distal end of bile duct. The advanced insulation coating helps prevent duodenal mucosal injury in EST. Guidewire operation is compatible with the long wire as well as with the short wire, allowing the guidewire to be controlled by an endoscopist or assistant. In addition, quick device exchange after guidewire retention is also possible.
Finally, some caution also be pointed out with this new device. Special technique may be required in EST as the knife being shorter. For instance, in EST of a large duodenal papilla, it is necessary to advance the catheter when performing an additional incision after incision from the proximal portion. In addition, the short knife tends to deform when bending frequently, so it may require to exchange.
We believe that the new short-bending CleverCut3V – which is now being popularized as the EST knife of choice in Japan – is a highly effective therapeutic accessory for WGC.
* Single Use Sphincterotome V (Distal Wireguided) KD-VC412Q-0215
References
- Takagi K, Ikeda S, Nakagawa Y, et al. Retrograde pancreatography and cholangiography by fiber duodenoscope. Gastroenterology. 1970; 59: 445-452.
- Kawai K, Akasaka Y, Murakami K, et al. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc 1974; 20: 148-151.
- Kawakami H, Maguchi H, Mukai T, et al. A multicenter, prospective, randomized study of selective bile duct cannulation performed by multiple endoscopists: the BIDMEN study. Gastrointest Endosc. 2012; 75: 362-372, 372.e1
- Kawakami H, Maguchi H, Hayashi T, et al. A prospective randomized controlled multicenter trial of duodenoscopes with 5 degrees and 15 degrees backward-oblique angle using wire-guided cannulation: effects on selective cannulation of the common bile duct in endoscopic retrograde cholangiopancreatography. J Gastroenterol. 2009;44:1140-1146.
- Kawakami H, Kubota Y, Ban T. Novel short curved sphincterotome for wire-guided cannulation and endoscopic sphincterotomy. Dig Endosc. 2018; 30: 400-402.
- Content Type