Disclaimer
The techniques and clinical opinions presented in this material reflect the personal experience and professional judgment of the healthcare professional and do not necessarily represent the views of Olympus. This material is intended for healthcare professionals only. Users should always refer to the applicable Instructions for Use (IFU) and use Olympus products in accordance with the approved indications and local regulatory requirements. The healthcare professional presenting this material has been engaged by Olympus and compensated at fair market value for their services.
Pancreatobiliary case 1
Asst. Prof. Dr. Tomislav Bokun
Head, Interventional Gastroenterology Unit
Department of Gastroenterology, Hepatology and Clinical Nutrition
University Hospital Dubrava,
Zagreb, Croatia
Scope: TJF-Q190V
Organ: Duodenum
Patient information: N/A
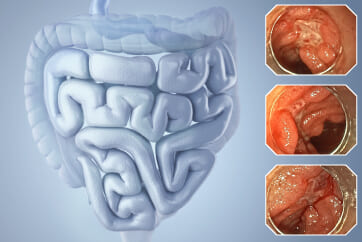
Medical history: Patient with choledocholithiasis, juxtapupillary diverticula and post-sphincterotomy bleeding
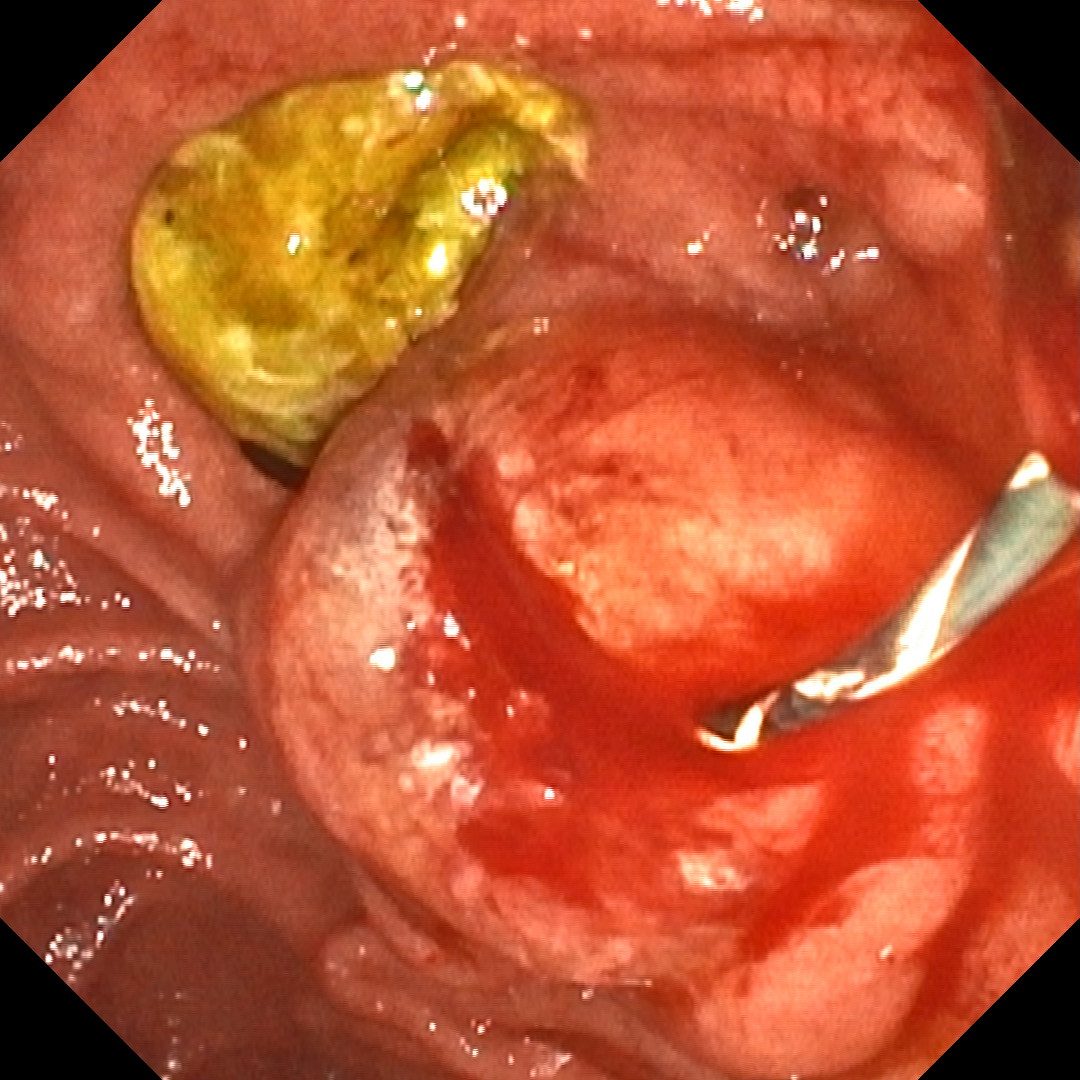
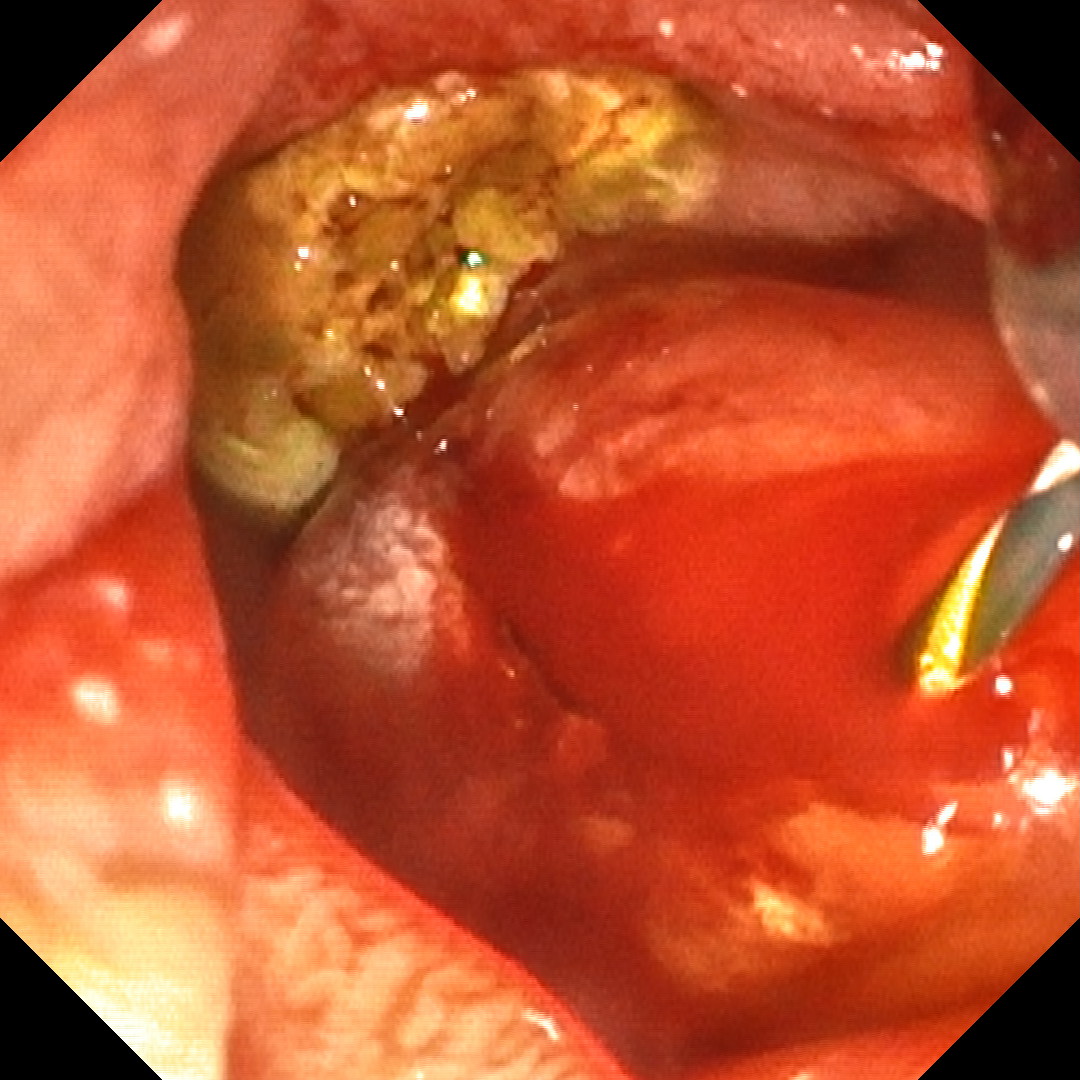
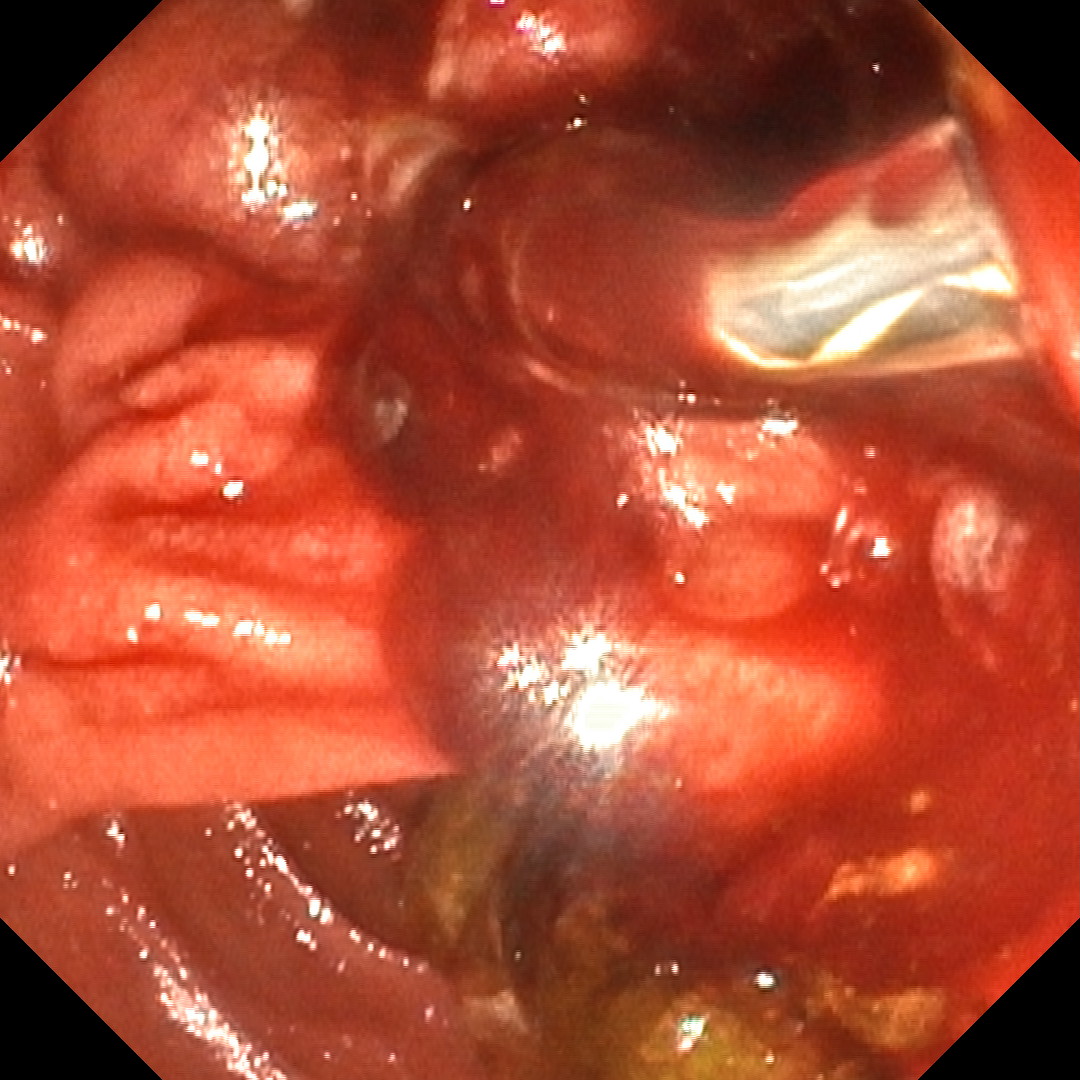
1. Bulging papilla -TXI2
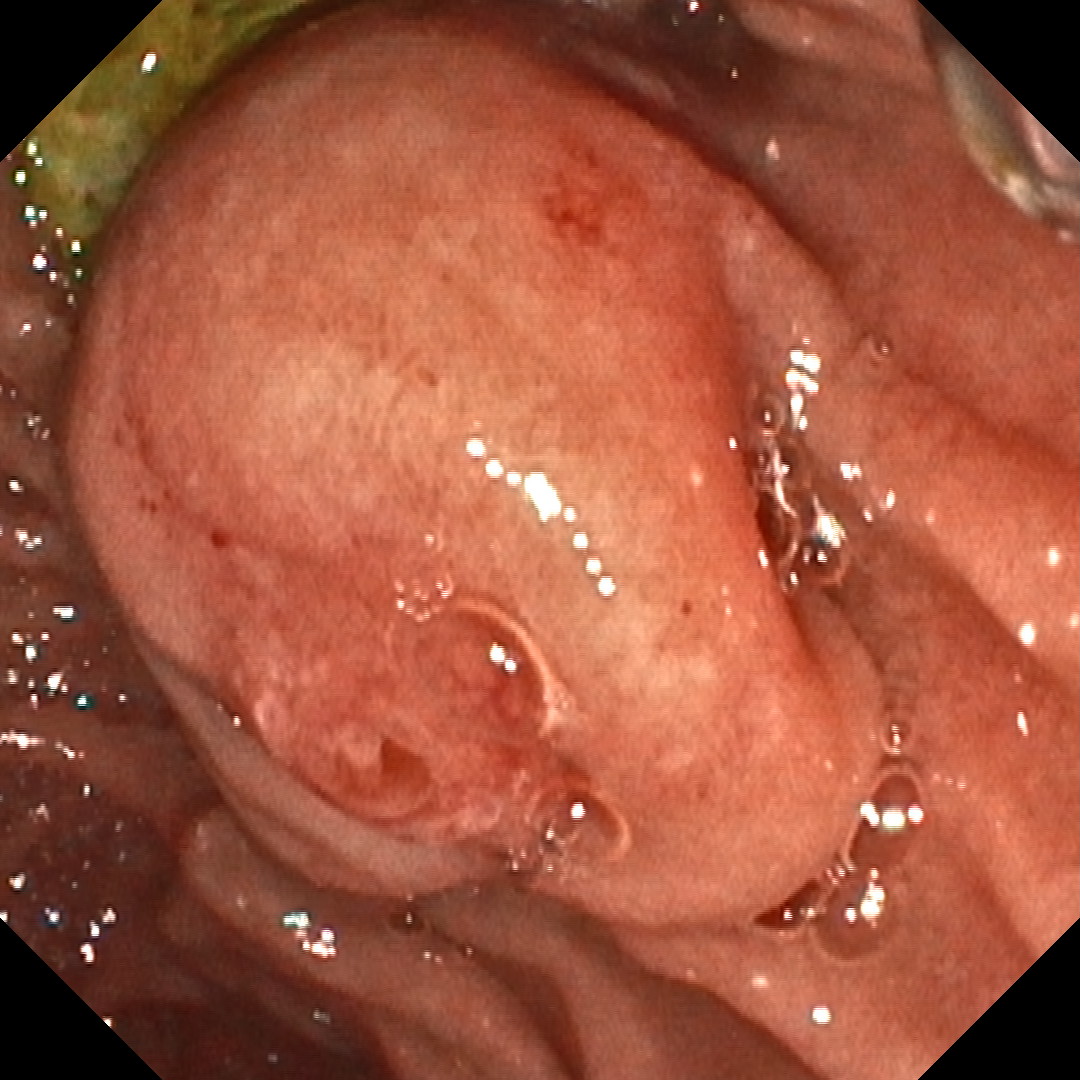
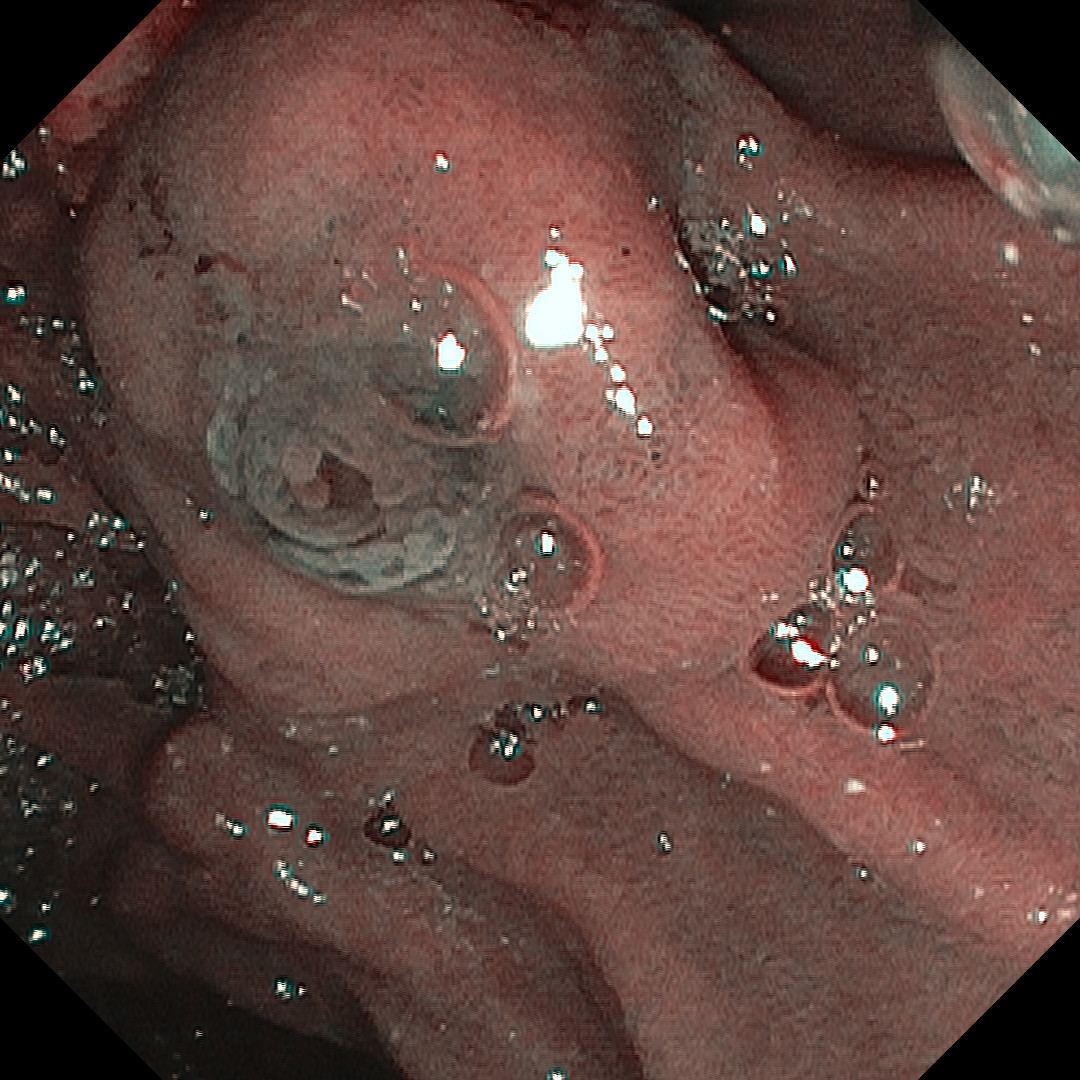
2. Bulging papilla - NBI
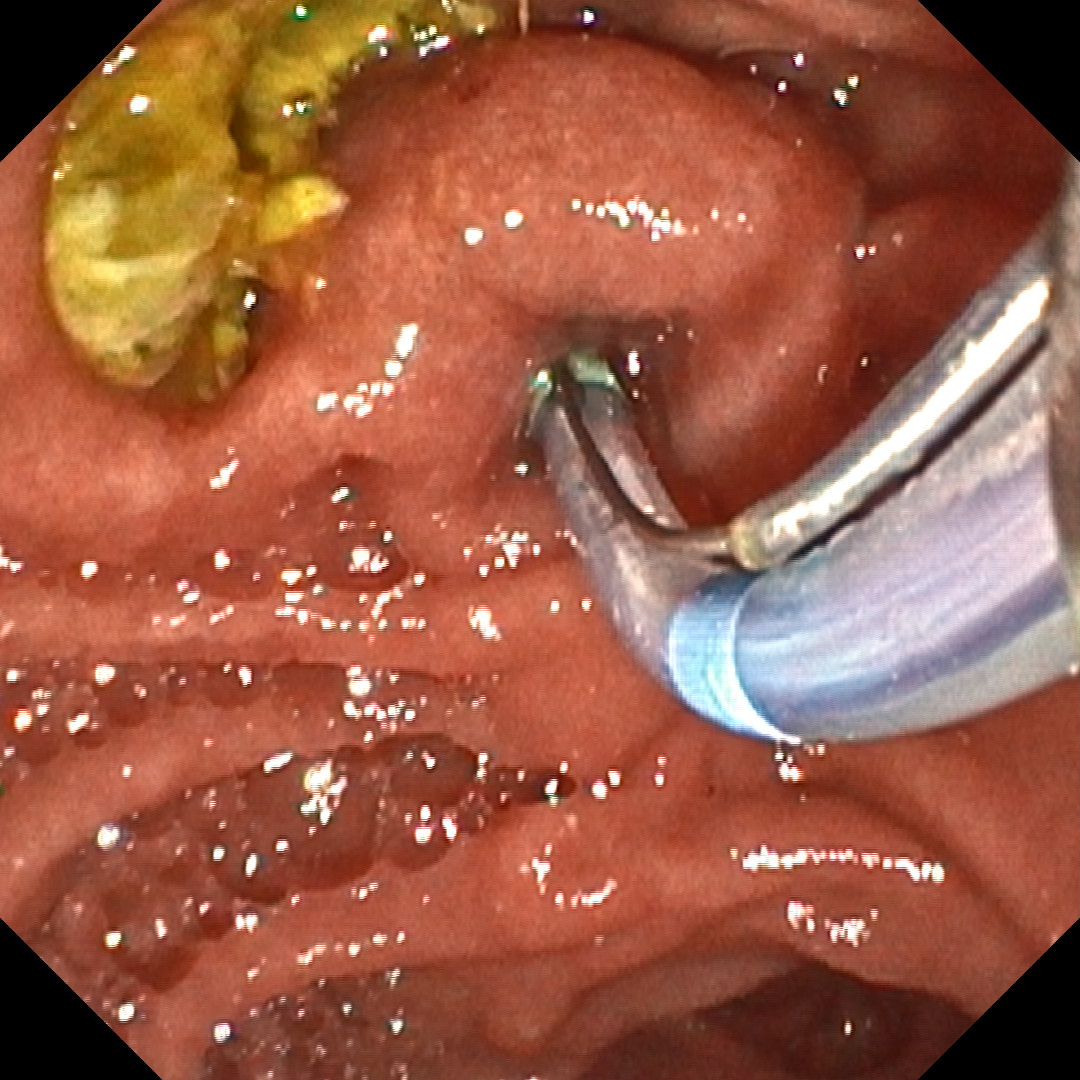
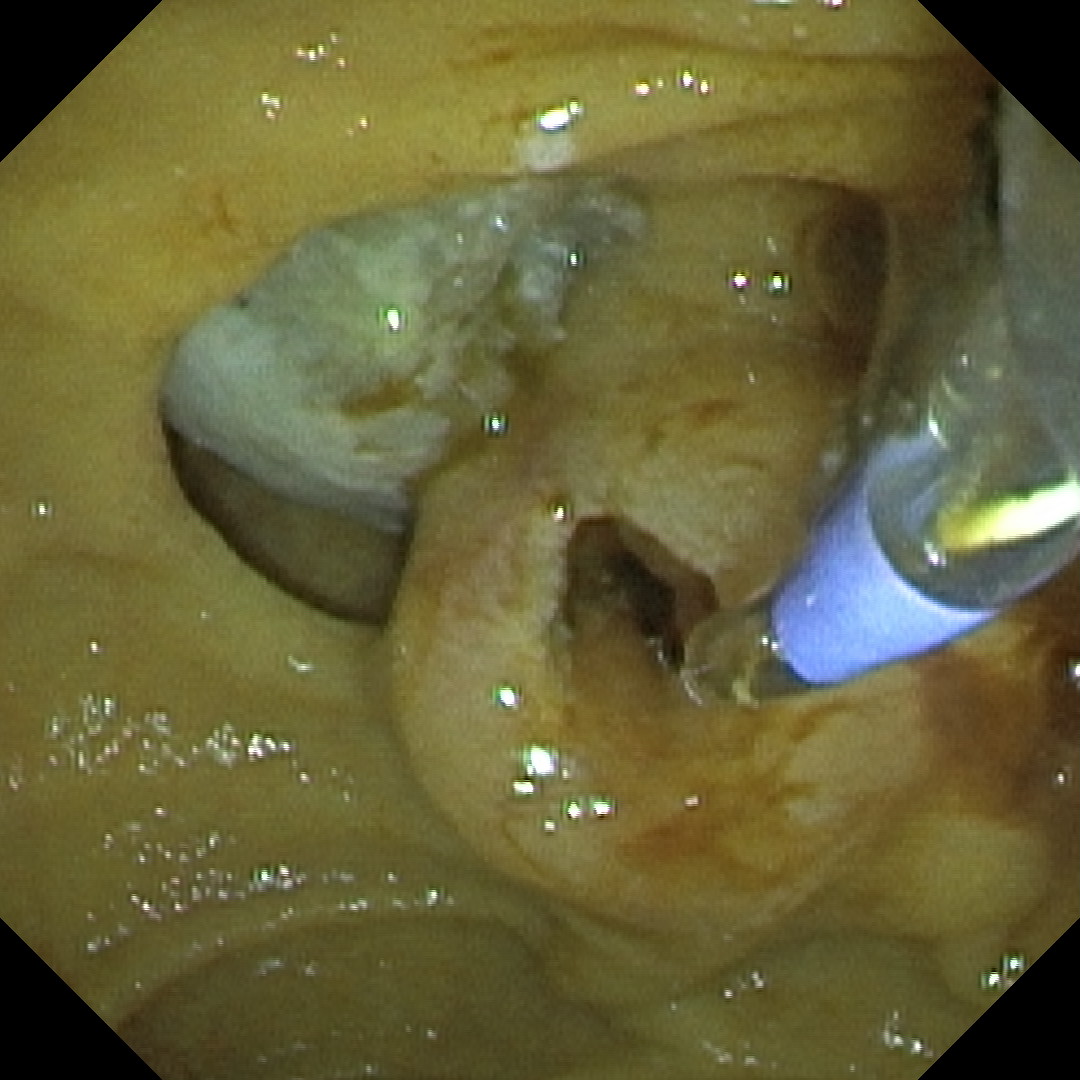
3. Cannulation
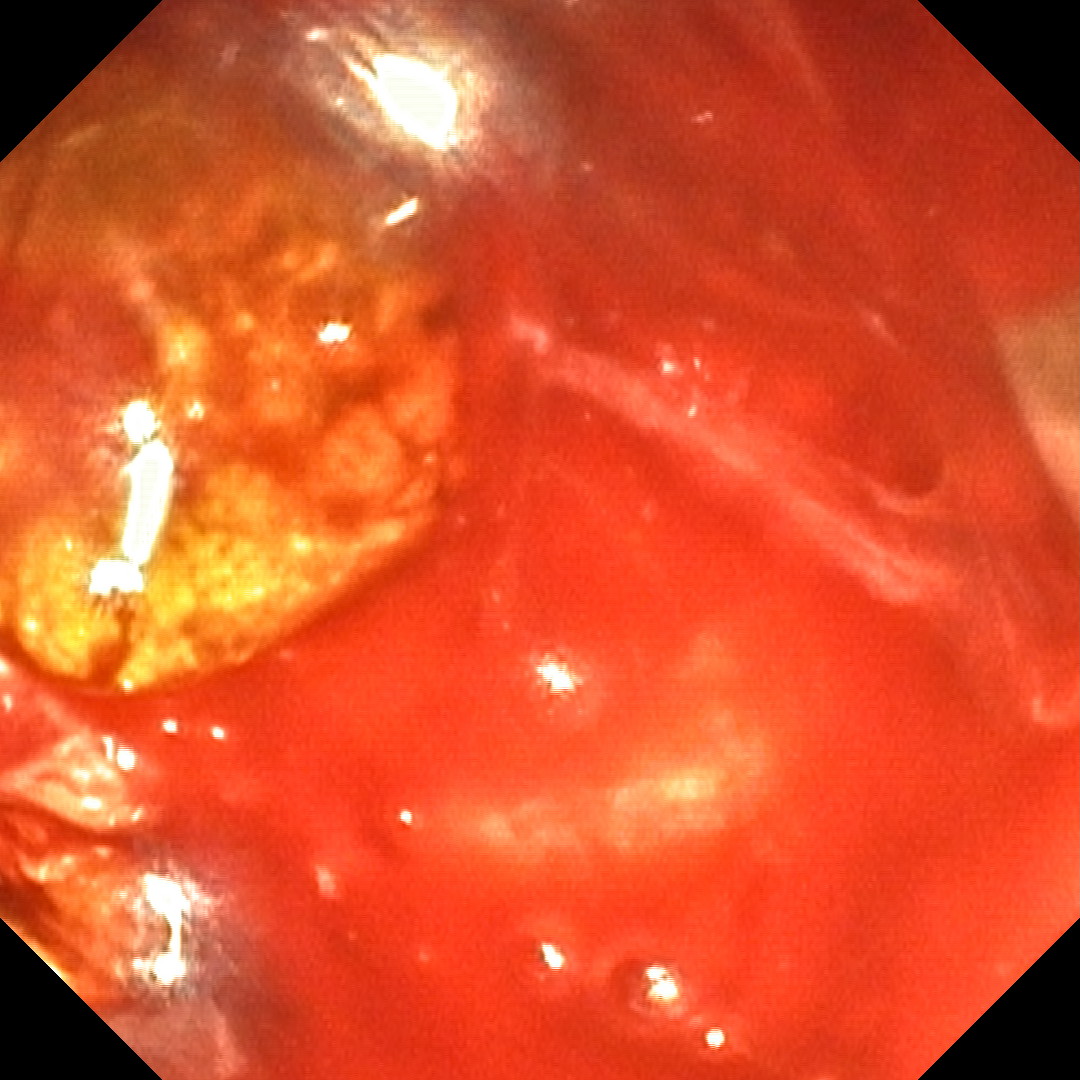
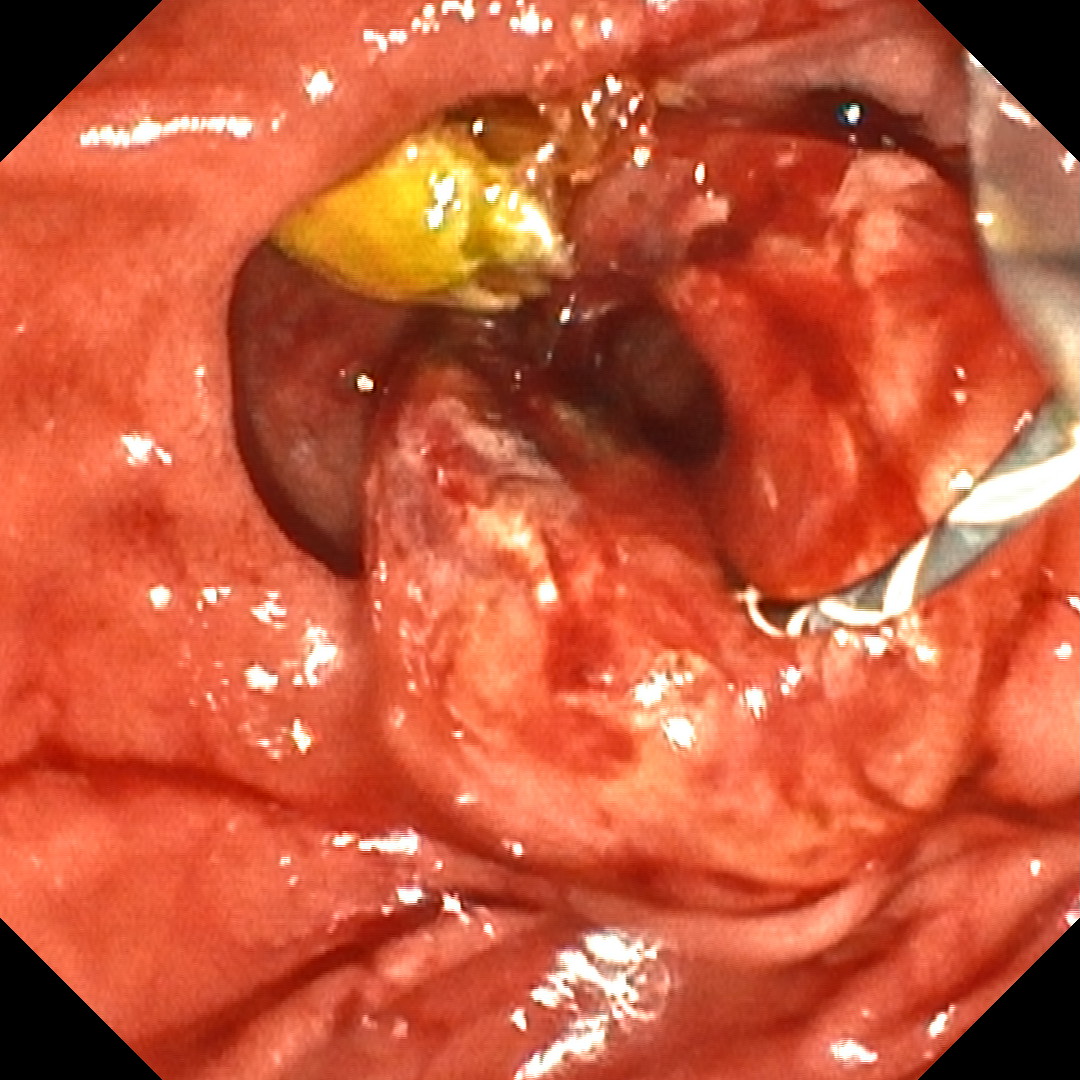
4. Post-sphincterotomy bleeding - TXI2

5. Post-sphincterotomy bleeding - RDI
6. Post-sphincterotomy bleeding - TXI2
7. Post-sphincterotomy bleeding - TXI2
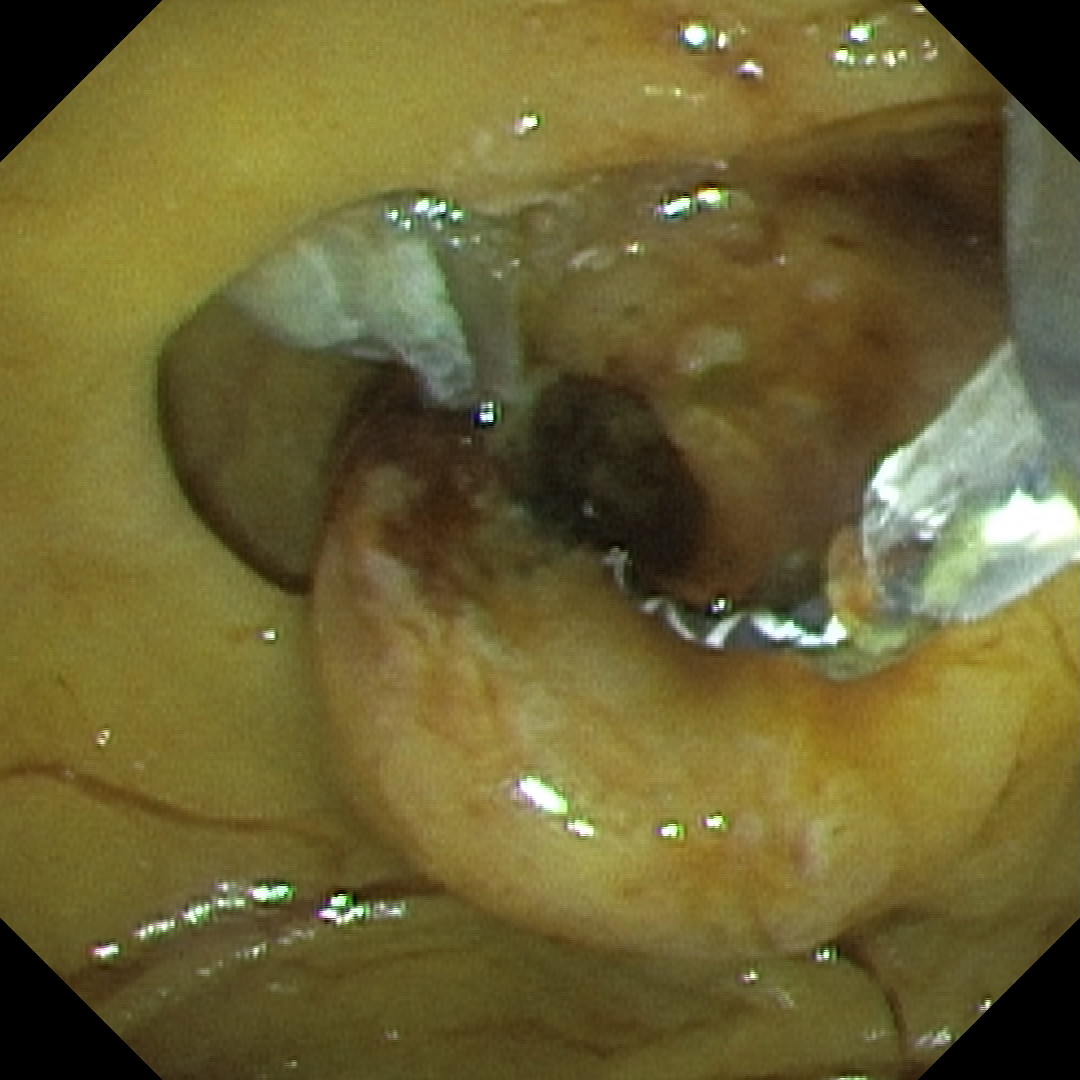
8. After electrocoagulation with sphincterotome - RDI
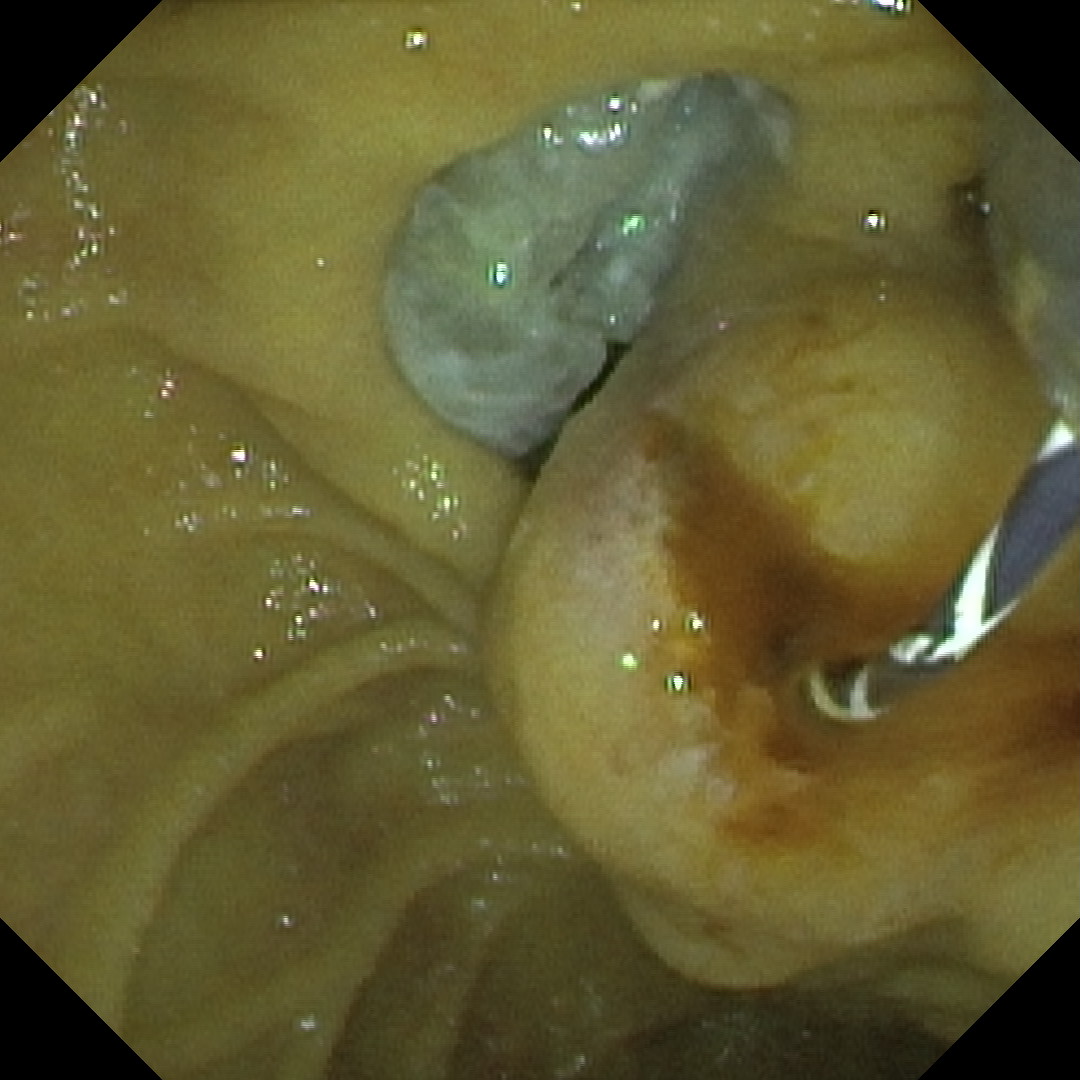
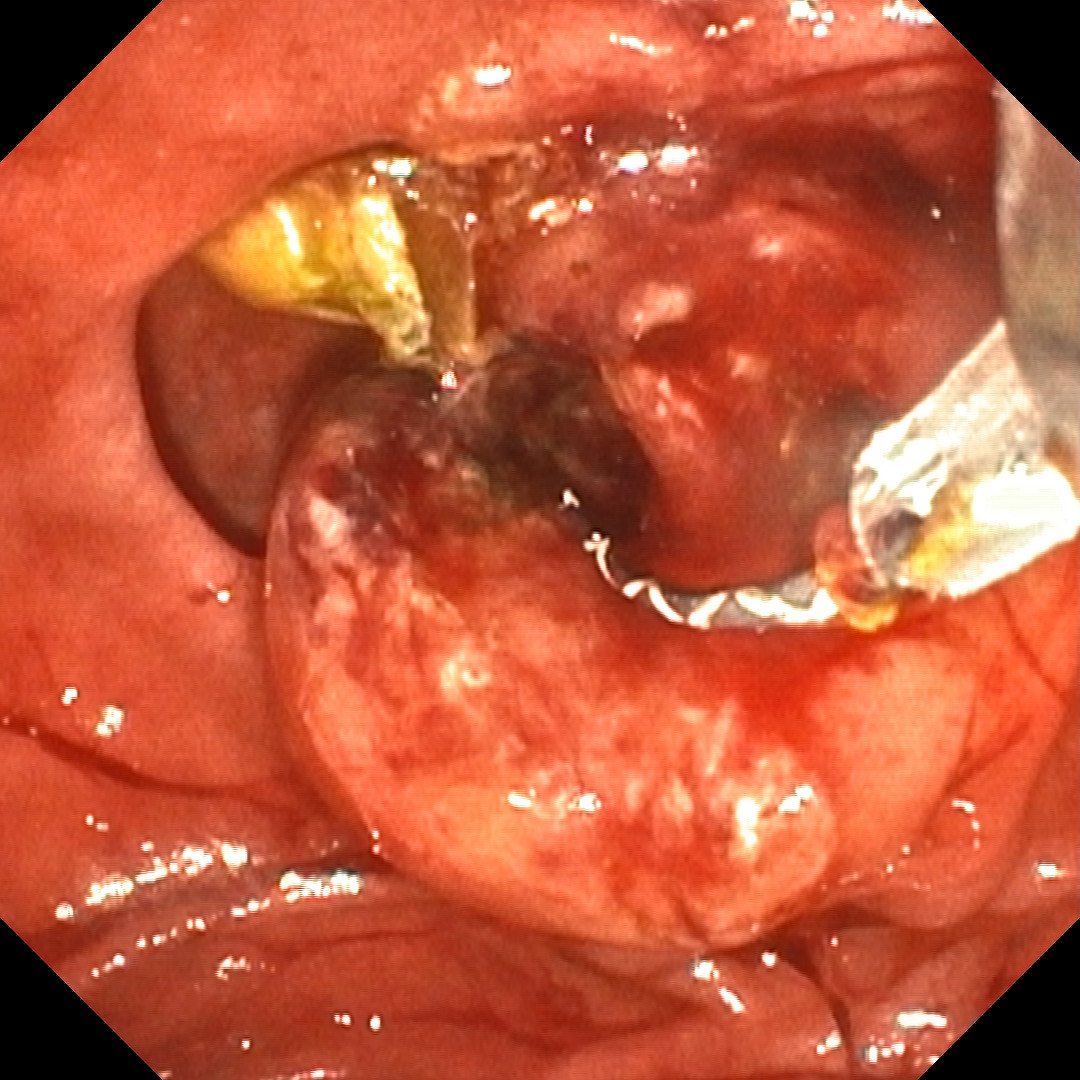
9. Stones extraction with bleeding recurrence - TXI2
10. Stones extraction with bleeding continuation - TXI2
11. Shrinking of bleeding after additional electrocoagulation with sphincterotome - TXI2
12. Further shrinking of bleeding after additional electrocoagulation with sphincterotome - TXI2
13. Bleeding stopped - RDI
Case Video
Overall Comment
This was a good example of using various imaging modes with an X1 processor and TJF‑Q190V. The patient, presenting with biliary obstruction and biliary-type pain, was shown by EUS to have multiple common bile duct stones and was referred for ERCP. During the procedure a periampullary diverticulum containing residual food was observed and partially cleared. The papilla was clearly identifiable and appeared enlarged with suprapapillary bulging, suggesting stones.
In my clinical practice I regularly use TXI to help identify the papilla. Once located, I assess it in WLI and TXI, and I always use NBI briefly to further exclude adenoma. In this series of images and video, TXI (here TXI2) precisely delineates the orifice. I often use TXI for cannulation because it emphasizes surface texture and gives a more “3D” appearance than WLI. Also, during aspiration, interference of bile is neglectable in TXI mode in comparison to reddish color of bile with NBI, impeding analysis and precise accessories insertion for canulation. Another useful mode is RDI, which in this case identified the exact site of post-sphincterotomy bleeding, allowing precise electrocoagulation with the sphincterotome targeted only to the bleeding site. Before RDI, it was often difficult to treat only the bleeding spot after post-sphincterotomy bleeding, and we frequently needed to coagulate both sides of the sphincterotomy line. With RDI we could target our treatment specifically to the bleeding point. Post-treatment inspection with WLI or TXI is necessary but can be challenging because of residual blood and coagulum; RDI helps detect active flow, even when subtle. After stone extraction a rebleed occurred, and again RDI-guided electrocoagulation with the sphincterotome successfully stopped the bleeding.
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer