Colorectal Case 26

Dr. Shiaw-Hooi Ho
Associate Professor of Medicine at the Department of Medicine,
Universiti Malaya, Malaysia
Disclaimer:
NBI™ and TXI™ technologies are not intended to replace histopathological sampling as a means of diagnosis
The positions and statements made herein by Dr. Ho Shiaw Hooi are based on Dr. Ho Shiaw Hooi’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
- Data on file with Olympus (DC00489968).
- Data on file with Olympus as of 07/17/2020.
Scope: PCF-H190DL
Organ: colon
Patient information: M, 80s
Medical history: Known dyslipidemia; complained of dyspepsia but was found to have positive fecal occult blood test
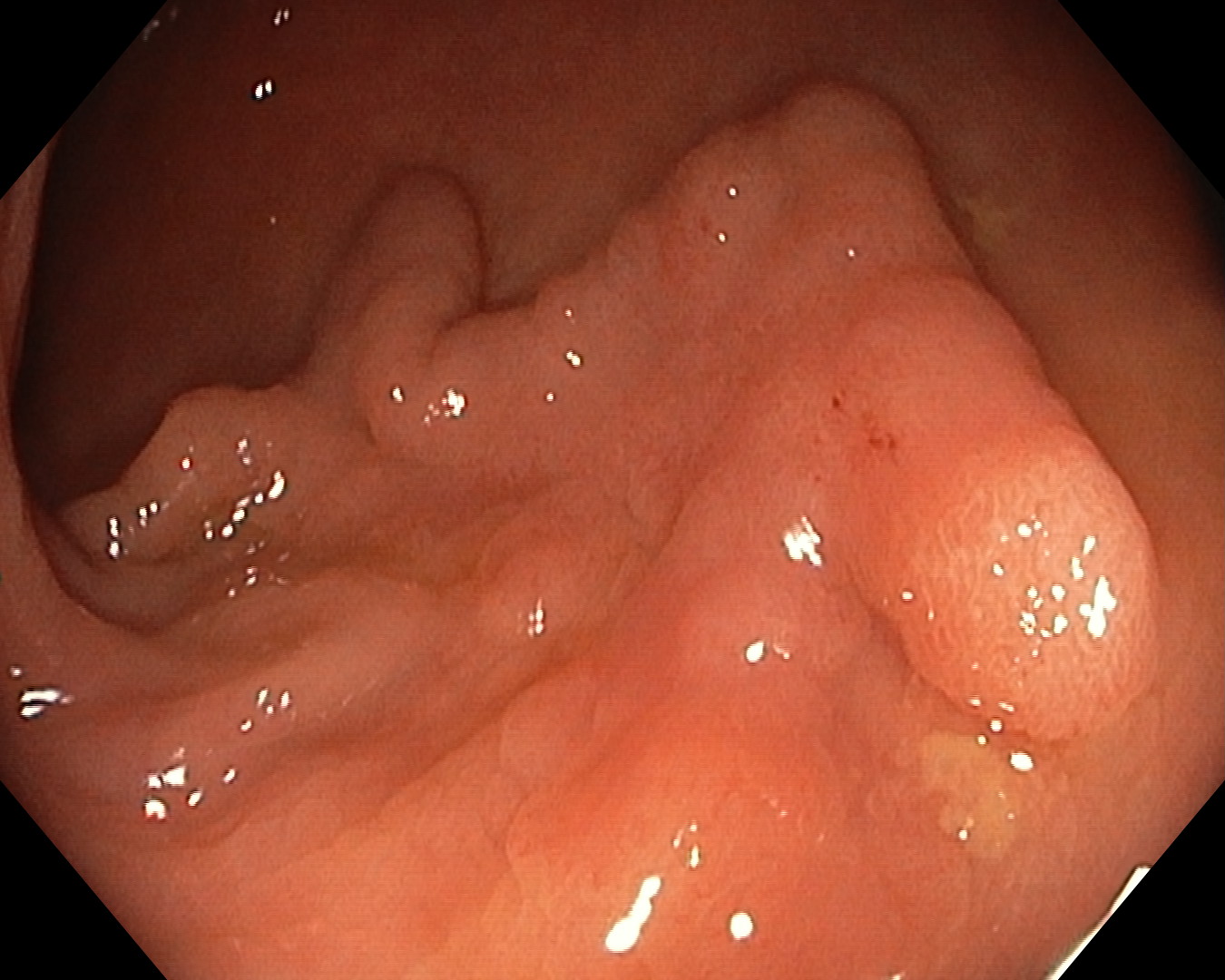
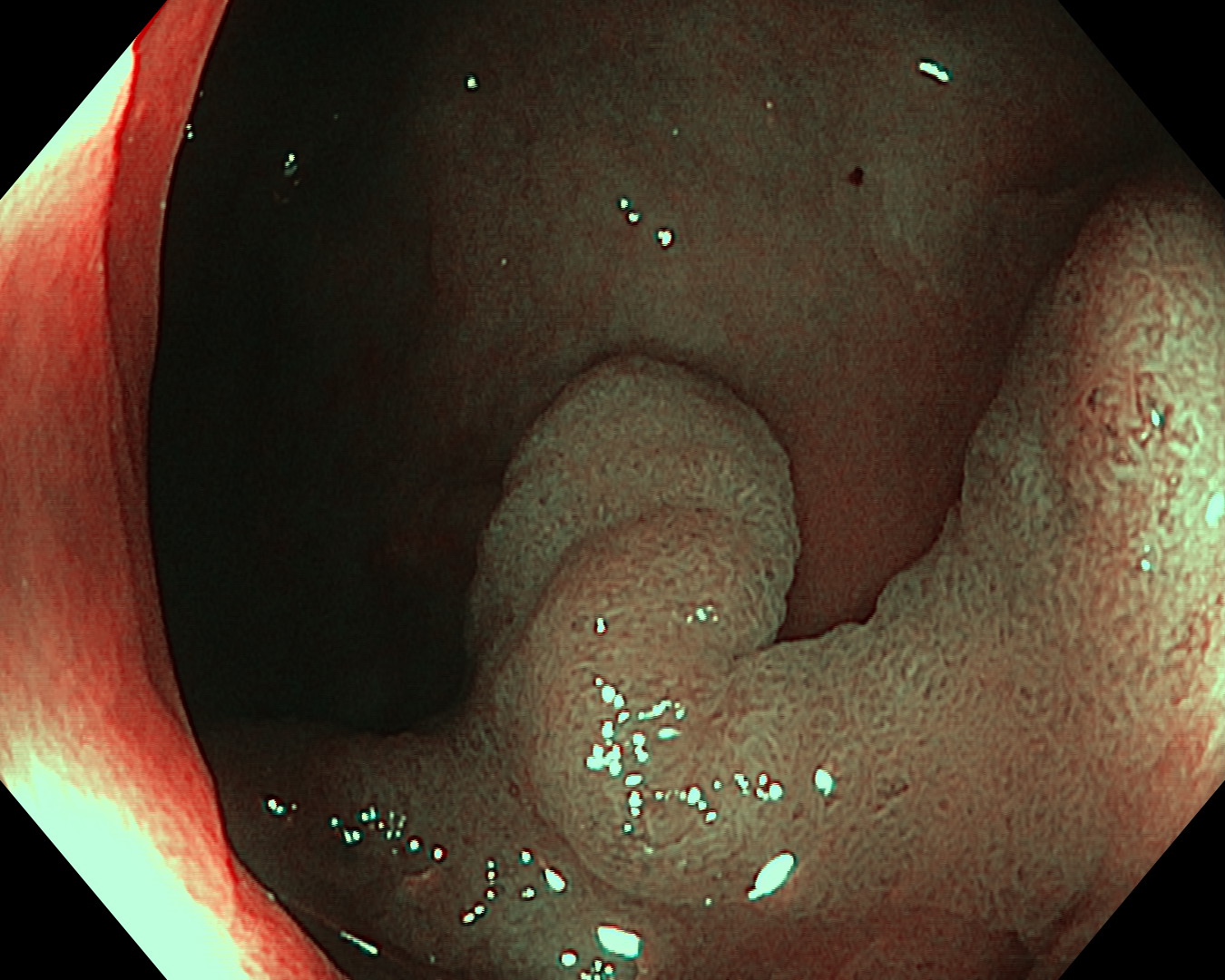
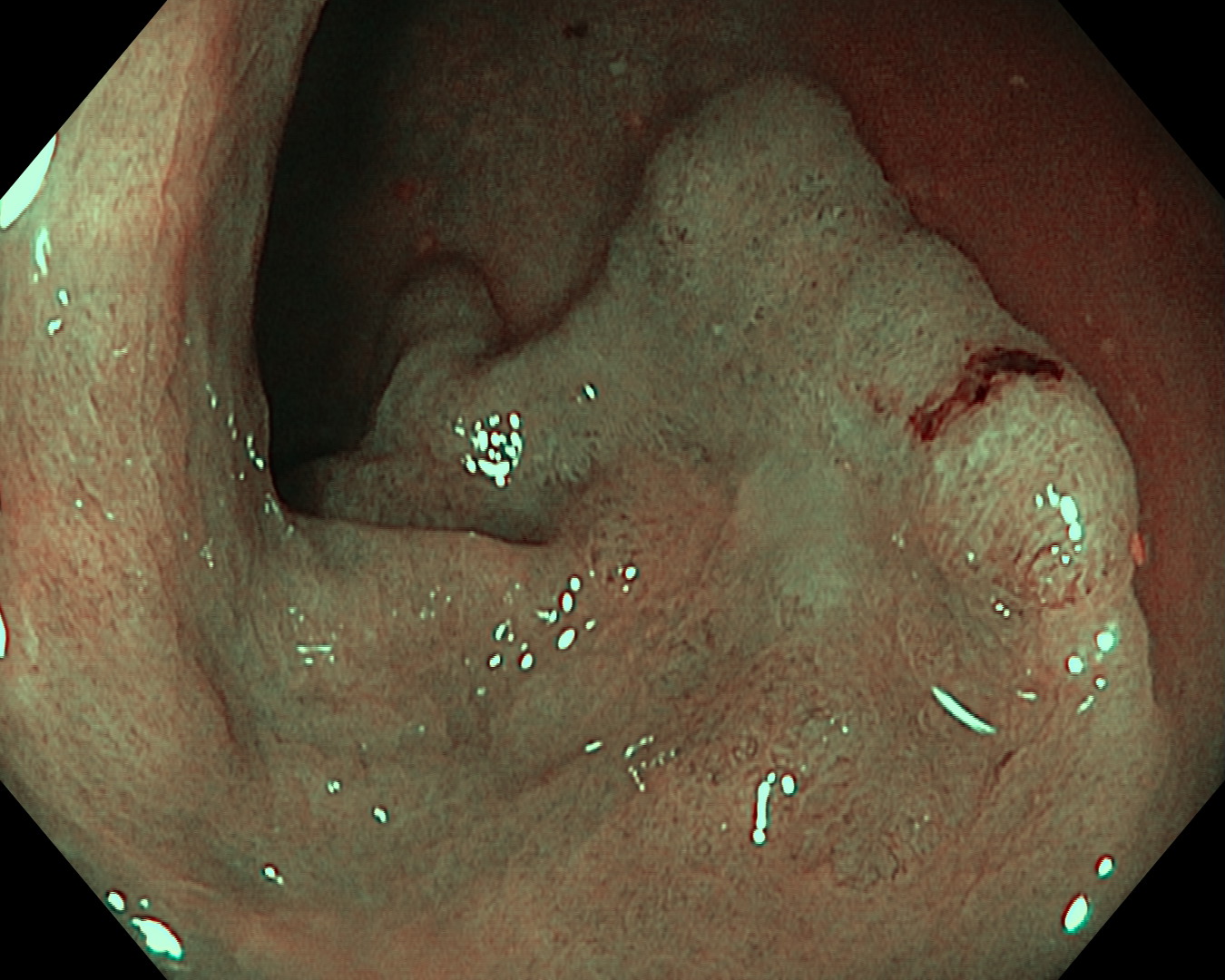
1. WLI Observation
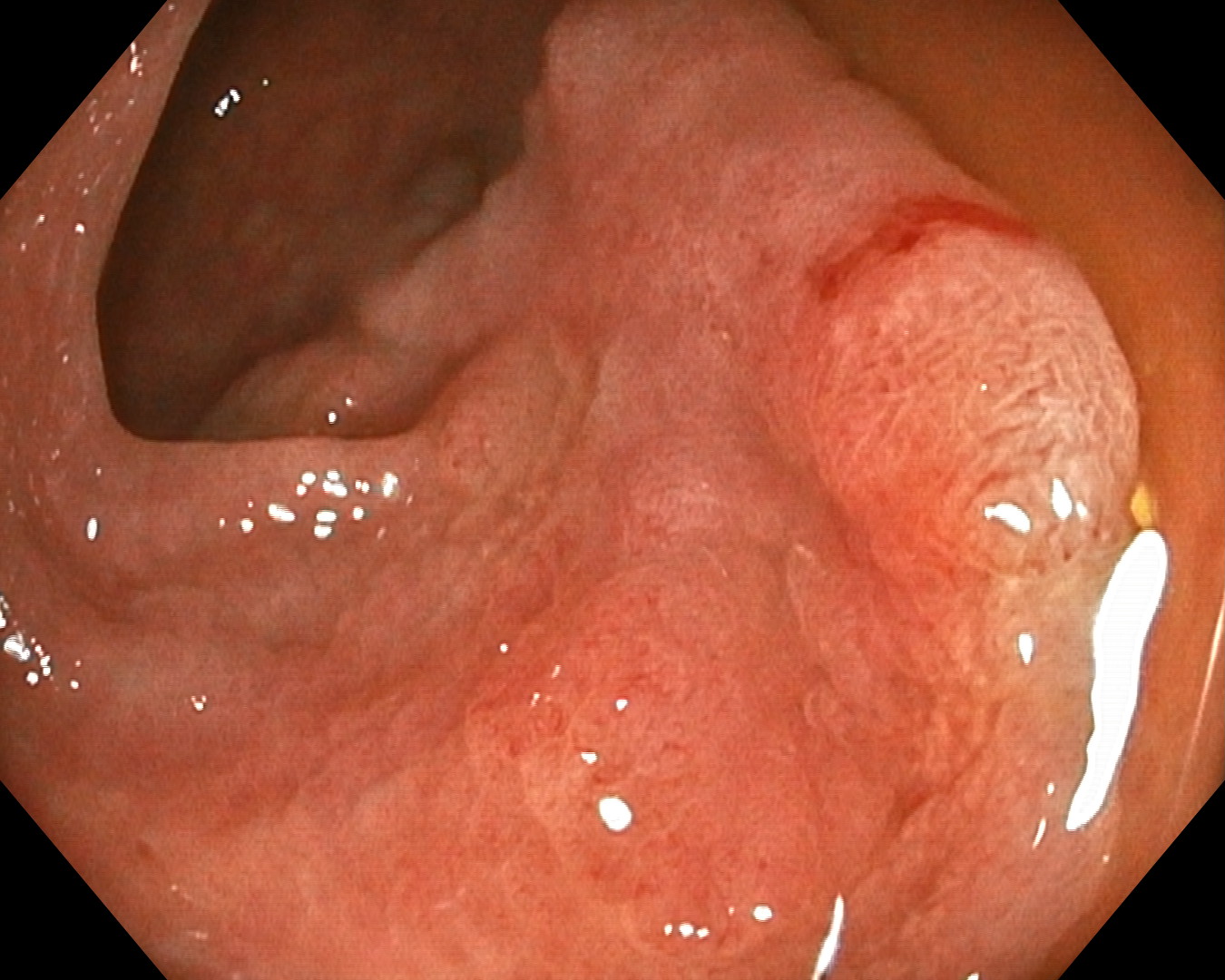
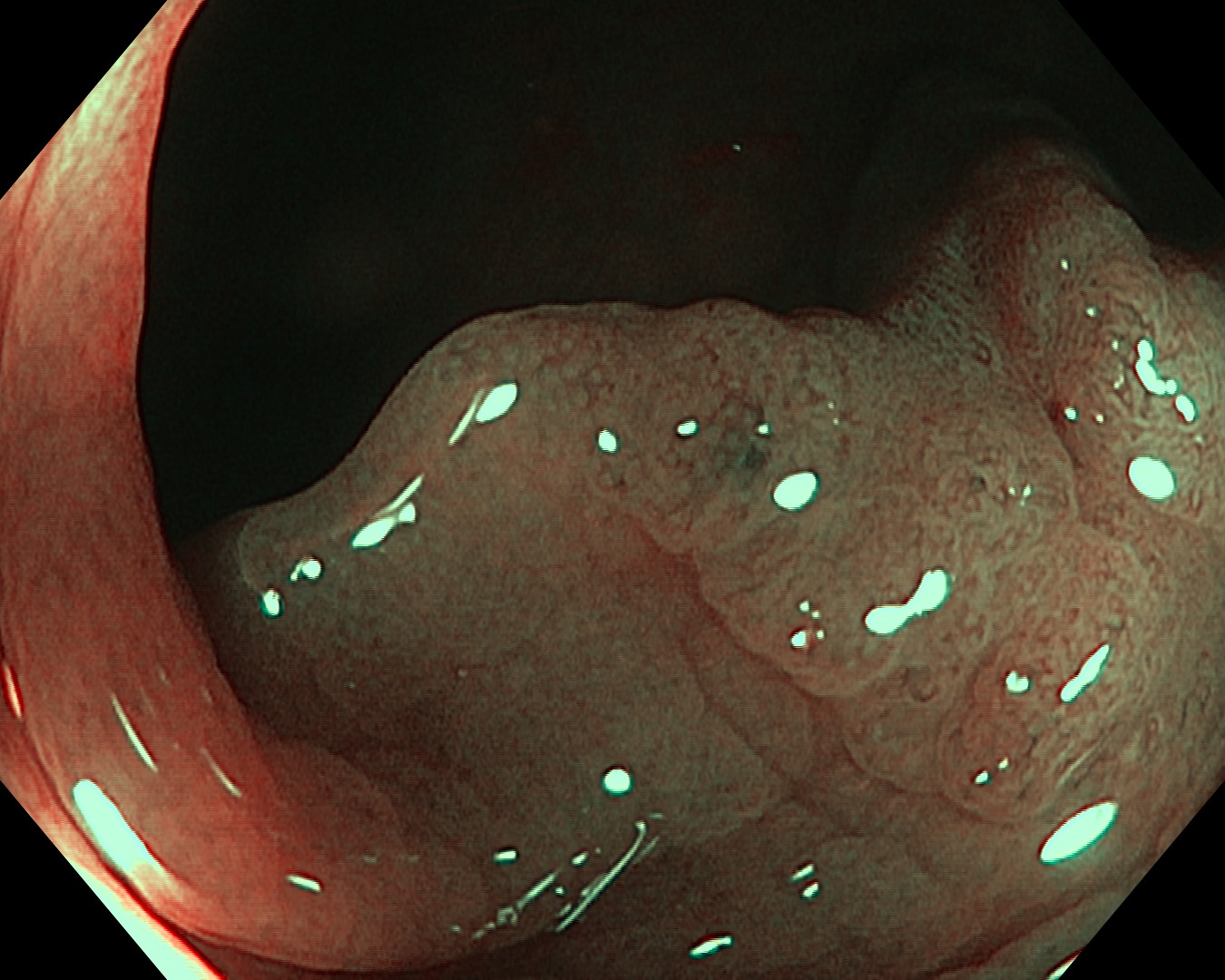
2. TXI™ technology Observation
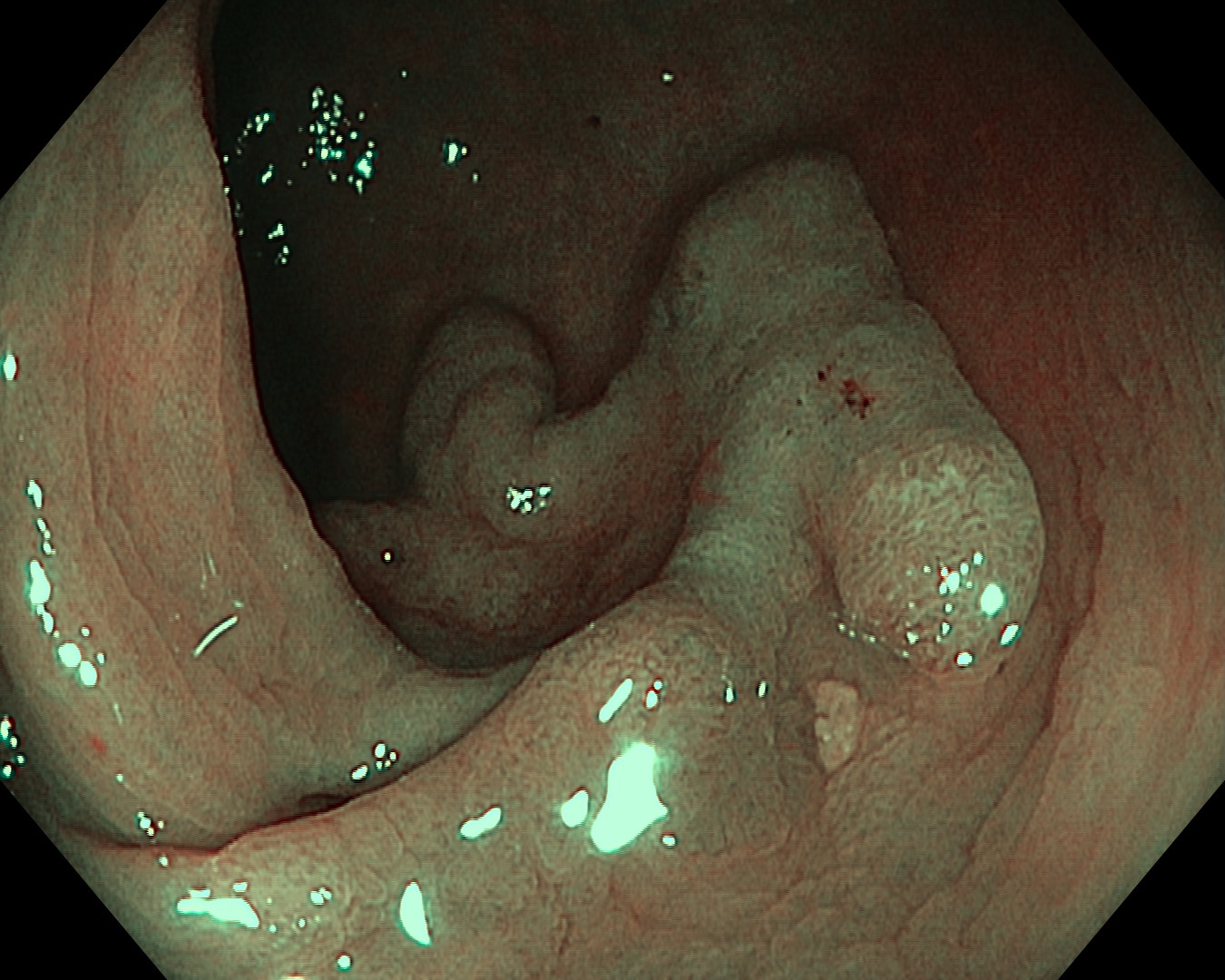
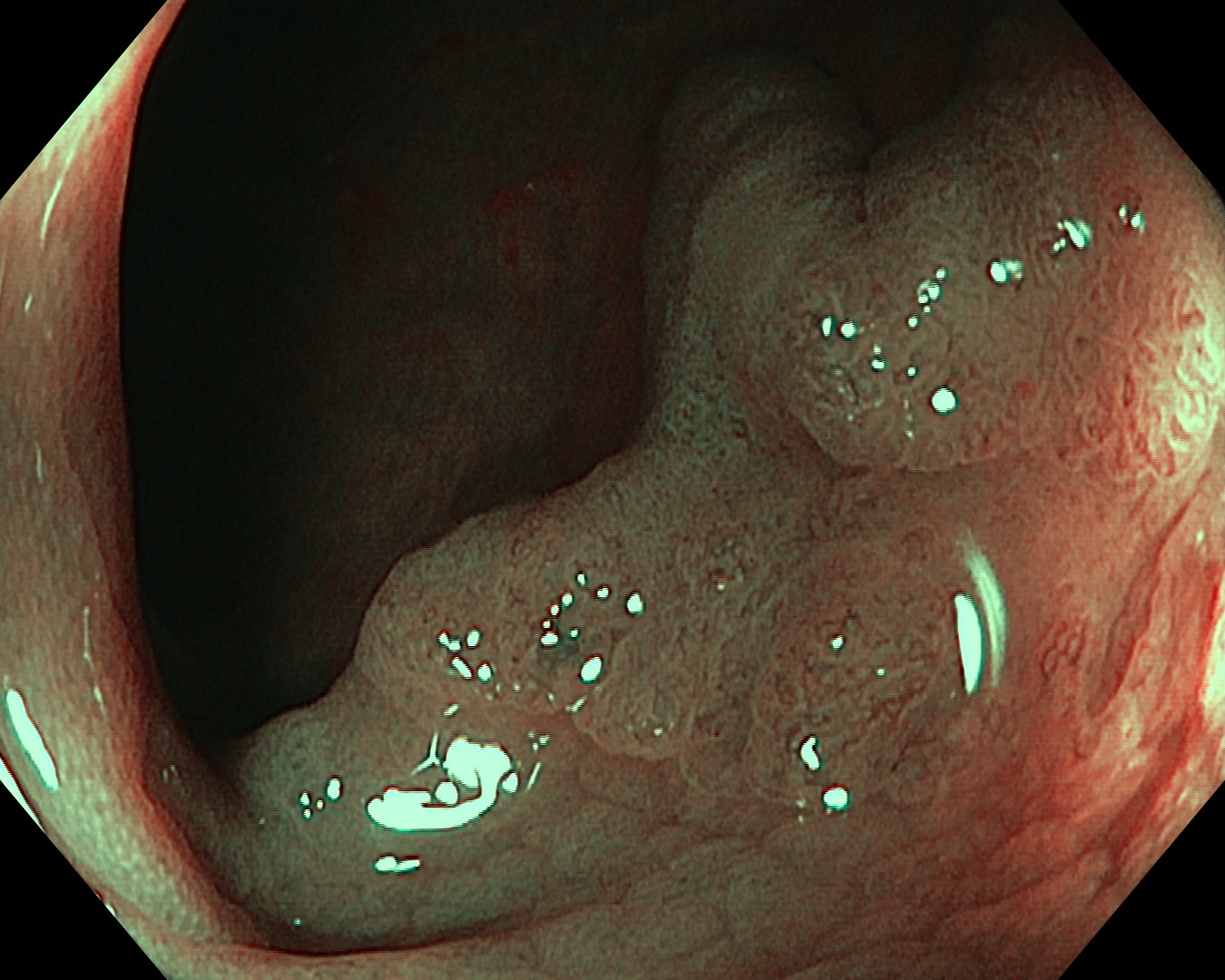
3. NBI™ technology Observation
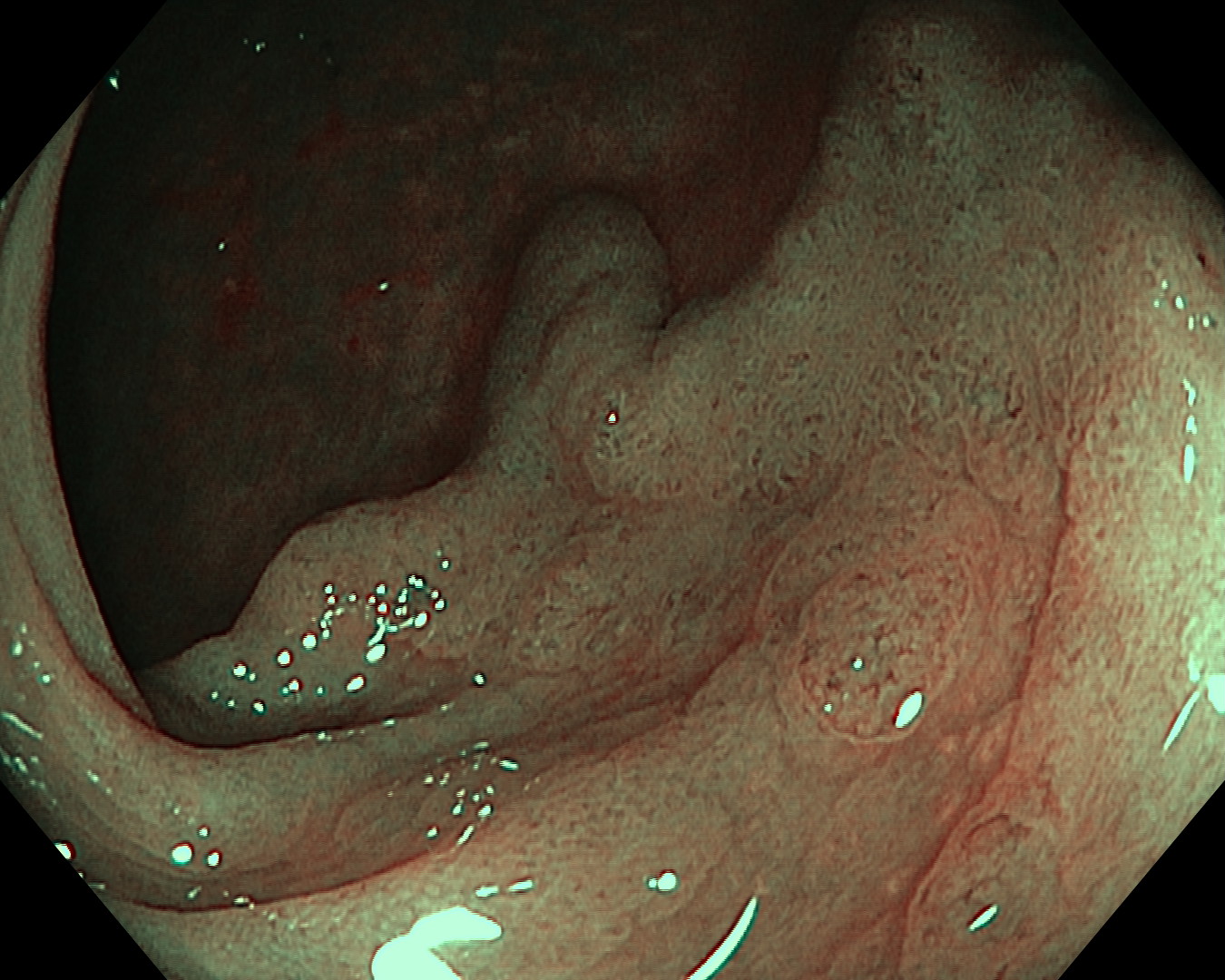
4. NBI™ technology Observation
5. NBI™ technology Observation
6. NBI™ technology Observation
7. NBI™ technology Observation
8. NBI™ technology Observation
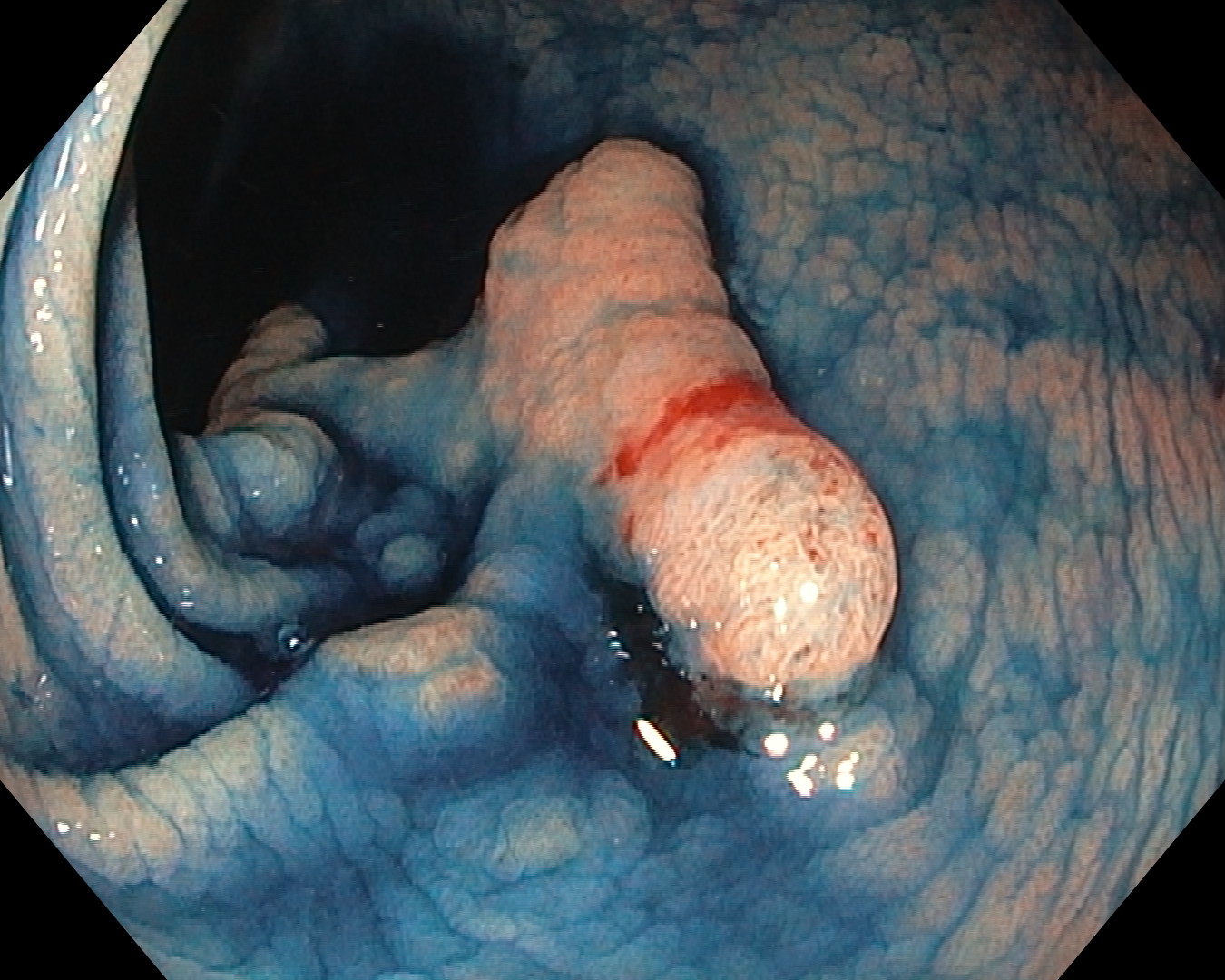
9. Indigocarmine Chromoendoscopy
Case Video
Overall Comment
The lesion was a flat elevated non-granular lateral spreading tumor measuring about 40mm at around the splenic flexure. Part of the lesion had indistinct border. Despite the inability to perform near focus examination due to the choice of colonoscope, close-up view under NBI™ technology mode was able to show a detailed image of this lesion and it helped in border delineation and recognition of the superficial vessel type under JNET classification.2 Conventional chromoendoscopy using indigo carmine dye further aided the border delineation. This lesion will be subjected for endoscopic submucosal dissection.
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer
- Content Type