Supervisor
Dr. Haruhiro Inoue
Showa University Koto Toyosu Hospital, Digestive Disease Center
Disclaimer: The positions and statements made herein by Dr. Inoue are based on Dr. Inoue’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
1. WHAT IS POEM
Achalasia is a primary esophageal motility disorder. A-chalasia means "no relaxation" in Greek. The main symptoms of achalasia are dysphasia (Swallowing difficulty), regurgitation of undigested food and chest pain. Dysphagia tends to become worse slowly but progressively.
POEM (Per-Oral Endoscopic Myotomy) is a newly developed endoscopic procedure intending eternal cure from the disease. In POEM procedure esophageal myotomy is done similar to conventional surgery, but with no incision.
Several thousand cases in various grades of achalasia received POEM procedure worldwide. Clinical results are excellent with no major complications with skillful doctors' hands.
2. EQUIPMENT
TriangleTipKnife™ J Device (KD-645L)
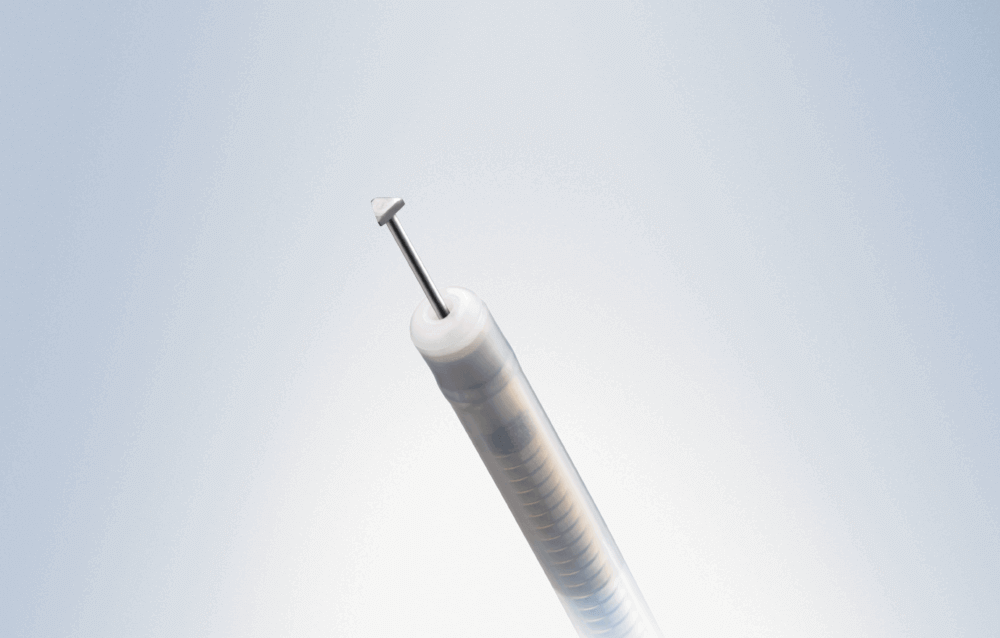
| Model | Min. working channel Ø | Working length | Cutting knife length | Cutting knife diameter | Triangular tip length | Triangular tip thickness | Sterile, single-use | Built-in handle |
|---|---|---|---|---|---|---|---|---|
| KD-645L | 2.8 mm or more | 1,650 mm | 4.5 mm | 0.4 mm | 0.4 mm | 0.3 mm | Yes | Yes |


Setting for Electrosurgical unit ESG-300
| Procedure | Mode | Power [w] | Effect |
|---|---|---|---|
| Incision | PulseCut slow | 30 | 2 |
| Dissection | SprayCoag | 30 | 3 |
| Myotomy | SprayCoag | 30 | 3 |
| Hemostasis by knife | SprayCoag | 30 | 3 |
| Hemostasis by Coagrasper | SoftCoag | 50 | 2 |
Caution: The following settings are examples based upon previous clinical usage of the device. Please note that clinical staff are solely responsible for selection of an appropriate mode and power level, dependent upon the instrument being used and the condition of the tissue being treated. Due to the heterogenicity of instruments and clinical confidence. Olympus cannot accept liability for clinical risks arising from the use of these example settings.
Related Devices
| Items | Quantity |
|---|---|
| EVIS EXERA™ III Video System Center CV-190 | 1 |
| EVIS EXERA™ III Xenon Light Source CLV-190 | 1 |
|
EVIS EXERA II™ Gastroscope GIF-H180J or EVIS EXERA™ lll Gastroscope GIF-HQ190 / H190 |
1 |
| EVIS EXERA™ lll Gastroscope GIF-XP190N | 1 |
| Electrosurgical unit ESG-300 / 400 | 1 |
| Endoscopic CO2 regulation unit UCR | 1 |
| Low flow tubing for UCR MAJ-1742 | 1 |
| Single Use Electrosurgical Knife TriangleTipKnife™ J device KD-645L | 1 |
| Coagrasper™ device FD-411UR | 1 |
| Distal Attachment MH-588 | 1 |
| Injection Needle NM-610L-0426 | 1 |
| Hemostasis Clip HX-202LR | 2 |
| Hemostasis Clip (Long arm) HX-201LR-135L | 15 |
3. OPERATOR QUALIFICATIONS
This procedure requires advanced endoscopic skills and should be done with the collaboration between expert endoscopists and expert surgeons. It is also highly recommended to perform the POEM under the guidance of experienced medical doctors especially for initial several cases.
4. PRETREATMENT AND ANESTHESIA
4.1 Pretreatment
4.2 Anesthesia
(1) General anesthesia with controlled ventilation (positive pressure) is required. That means the procedure should be done under control with anesthesiologist.
(2) In a patient with dilated esophagus esophageal content should be cleared with therapeutic endoscope. It potentially avoids aspiration pneumonia during intubation.
5. PREPARATION
5.1 Patient Position
(1) Supine Position
(2) Expose the patient belly (upper abdomen) to check the pneumoperitoneum quickly.
(3) 8% patient of all cases becomes pneumoperitoneum during procedure.
5.2 Configuration
(1) General anesthesia with intratracheal intubation is required. That means the procedure should be done under control of anesthesiologist.
(2) All endoscopic devices should be sterilized with ethylene oxide gas (EOG).
- Keyword
- Content Type