1. Introduction
Now Olympus has introduced the highly anticipated system “EVIS X1” for bronchoscopy.
EVIS X1 is designed to support advanced diagnosis and therapeutic treatment of bronchial diseases through a series of visualization and tracheobronchial access innovations that include BAI-MAC (Brightness Adjustment Imaging with MAintenance of Contrast), Red Dichromatic Imaging (RDI), and TeXture and Color Enhancement Imaging (TXI). Recently, Prof. Felix JF Herth at University of Heidelberg, Germany used the EVIS X1 system on a trial basis for several months. Today, Prof. Herth talks about how the current challenges of bronchoscopy affect his procedures and the improvements achieved with the use of EVIS X1 system.
This information is intended solely for the use of healthcare professionals. A healthcare professional must always rely on his or her own professional clinical judgment when deciding whether to use a particular product when treating a particular patient. A healthcare professional must always refer to the package insert, product label and/or instructions for use, including the instructions for cleaning and sterilization (if applicable), before using any Olympus product.

EVIS X1 System

EVIS X1 VIDEO SYSTEM CENTER
OLYMPUS CV-1500
2. Current Challenges and the Situation in Bronchoscopy
2-1. Brightness in Airway Anatomy
What is brightness adjustment?
Normally, when the scope is in the airway, the operator can only observe clearly what is in the near field. Brightness in the far field is typically insufficient, especially in large, long cavities, in turning anatomy, or in anatomy with protruding parts.
The further away from the scope, the darker the view, terminating in what essentially looks like a black spot.
As a result, if the endoscopist wishes to look deeper in the system, it will be necessary to move the scope in the direction of that black spot to better visualize the depths. Furthermore, if the scope is focused on the black spot, the entire view field will appear darker – irrespective of whether the endoscopist looks to the right, left, or into the depths – because the scope is actually focusing on the center position.
2-2. Visualization in Bronchoscopy
Obtaining a clear image of the mucosa, whose various shades of red are difficult to differentiate, can be challenging. Illumination inside the bronchial anatomy is crucial in order to also anticipate deeper structures. Dark areas need to become brighter without overexposing areas close to the bronchoscope tip. When this is achieved, it can enhance ease of use and potentially reduce fatigue.
As is well-known, NBI imaging enhances observation of the upper surface of the mucosa by making the vessels stand out more distinctly. Now that the technique has become widespread, it is a standard feature on new scopes.
The main drawback of NBI is that because it is designed for observing capillaries in the superficial layer it is limited to penetration into the mucosa. Internal bleeding in general can be a serious challenge. Consequently, prevention of bleeding during a bronchoscopy is crucial.
3. New EVIS X1 Technology
3-1. BAI-MAC (Brightness Adjustment Imaging with MAintenance of Contrast)
3-1-1. Principle of BAI-MAC and Its Application in Bronchoscopy
BAI-MAC splits the image into texture and brightness information, automatically enhancing the brightness of the dark area and combining that with the original texture information. This generates an image in which near and far areas are evenly illuminated, resulting in a clearer view within the bronchial structure.
3-1-2. Clinical Case (Severe dysplasia – 56 y, male)
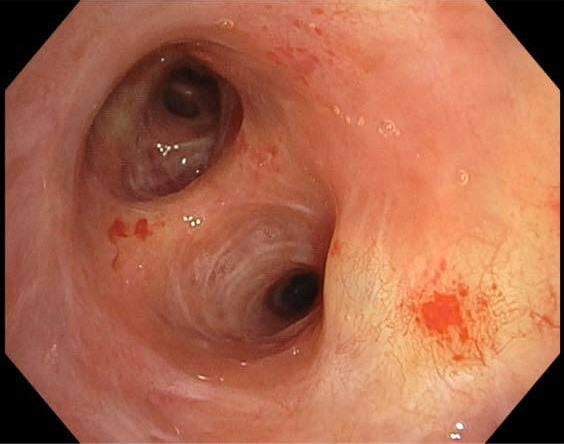
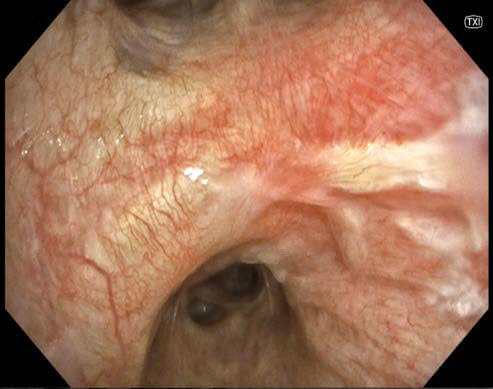
BAI-MAC ON
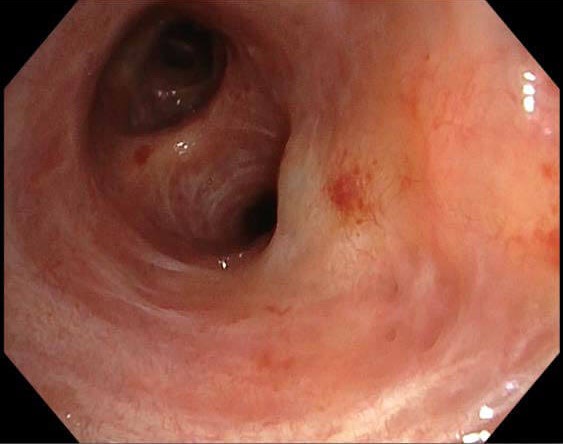
BAI-MAC OFF
This patient reported occasional bouts of very mild hemoptysis. A CAT scan showed nothing abnormal. Under bronchoscopy, a lesion was detected exhibiting severe dysplasia. It was decided to monitor the lesion and perform another bronchoscopy on the patient in three months.
BAI-MAC provides a better overview inside the anatomy, making it possible to take procedure quality and examiner confidence to the next level. When the BAI-MAC mode is turned on, the entire view field is significantly brighter, making it possible to observe much farther into the depths of the bronchi, improving the chances of detecting any anomalies.
3-2. TXI (TeXture and color enhancement Imaging)
3-2-1. Principle of TXI and Its Application in Bronchoscopy
TXI splits the white light into texture and base, while enhancing the brightness to stack them, then enhances the color tone to output. As a result, TXI emphasizes the mucosa’s texture and color, making tissue clearer and more three-dimensional, providing a more accurate and comprehensible view.
TXI takes a normal white light image, then analyzes the texture, the details, and the color, generating a realistic image with a noticeable three-dimensional feeling.
Two modes are available, one which enhances color and one which enhances texture, enabling the operator to experiment with different modalities to achieve a better visualization of the endobronchial image.
3-2-2. Clinical Case (Microinvasive cancer – 56 y, female)
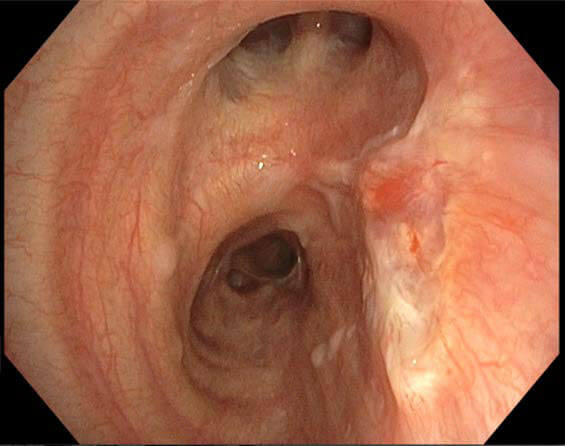
TXI OFF
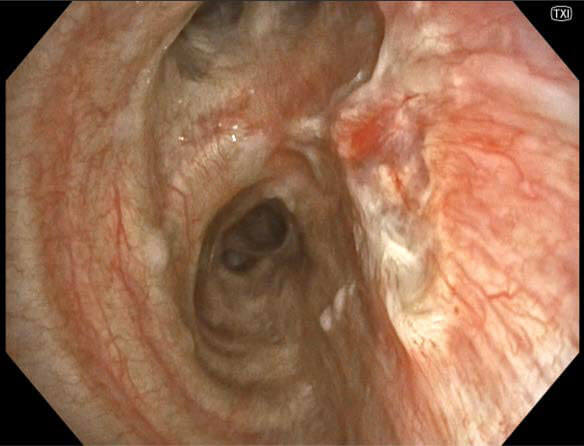
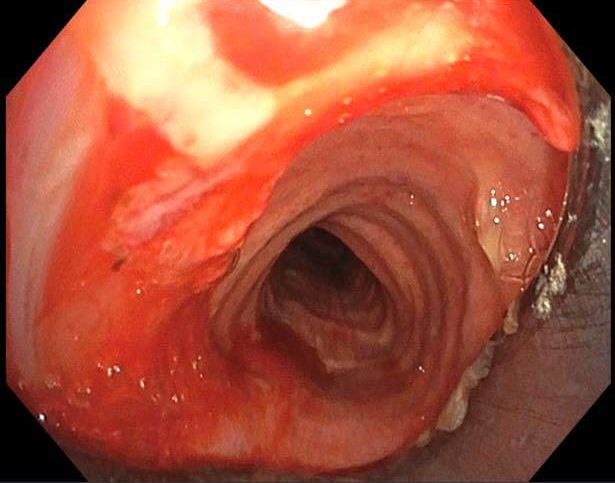
TXI ON
TXI ON
The patient came in with mild hemoptysis. Upon examination, an early cancer lesion was found. As it could not be determined initially whether there was any invasion, the question was whether to resect or ablate the tumor.
This made it all the more important to be able to see the margin of the lesion. The lesion was on the upper lobe carina on the right side. Potentially, this would require another sleeve resection, which would lead to loss of all function in the upper lobe. Consequently, being able to determine the extent of invasion was critical. To obtain the detailed view necessary to determine how to proceed, TXI was used.
Unfortunately for the patient, the TXI image showed change and pathologic revascularization up to the upper lobe carina. The tumor can be seen extending into the upper lobe carina. This clearly indicated a micro-invasive situation, requiring that the patient be offered a resection even though most of the tissue was healthy. In this case, failing to plan in advance and instead resecting just part of the right main bronchus could have led to having to perform repeated operations once the extent of the tumor was known. Planning in advance to perform an upper lobe sleeve resection resulted in a much better outcome.
3-3. RDI (Red Dichromatic Imaging)
3-3-1. Principle of RDI and Its Application in Bronchoscopy
Internal bleeding in general can be a serious challenge. Consequently, prevention of bleeding during a bronchoscopy is crucial.
Whereas NBI facilitates observation of capillaries in the superficial layer, RDI enables observation of large blood vessels in deeper layers.
RDI is designed to enhance the visibility of blood vessels in the deeper mucosal layers, as well as sources of bleeding.
NBI’s main drawback has always been its limited penetration into the mucosa. By combining an additional wavelength, in this case amber, which can penetrate further into the tissue, it is possible to visualize deeper mucosal layers and to look a little bit deeper into the epithelium.
These modes can be activated at the press of a button. The initial mode is the white light mode. Pressing the button activates the RDI mode, which provides an enhanced view of the vascularization that is clearer and easier to observe than in the standard white light mode.
3-3-2. Clinical Case (Web like tracheal stenosis – 26 y, female)

RDI ON
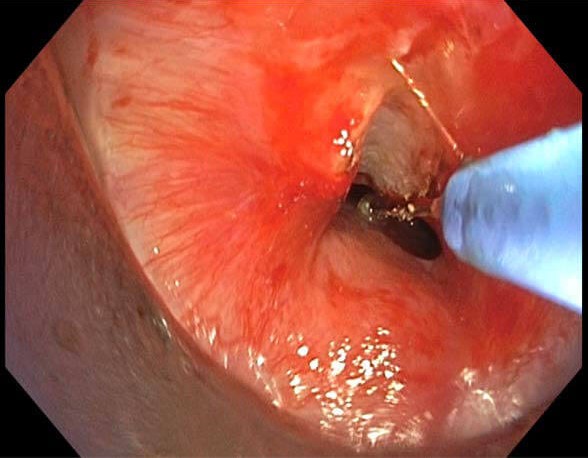
This patient presented with a web-like tracheal stenosis just below the vocal cords. The cause could not be determined. There was no disease. The biopsy was only a little fibrotic. The patient had never been intubated in the past.
To remove the stenosis, it was decided to use electro-knives to cut it and then to do the dilatation. To determined where to make the incision, RDI was used to observe the site.
This revealed the presence of vascularization and scarring. It was decided to do the incision at the point where there was more scarring.
The electro-knife was able to cut through the web-like area smoothly. There was no bleeding because with the help of RDI it was possible to see where the bigger vessels were and avoid them, ensuring that the incision could be performed safely.
As a result, the web-like area was reopened cleanly and the patient’s shortness of breath immediately became less severe. Thanks to RDI, it was possible to observe and analyze the vascular area, which in turn made it possible to determine where to place the electro-knife, where to make an incision and perform the resection.
4. New EVIS X1 Bronchoscopes
4-1. Slim Outer Diameter and Bigger Instrument Channel

BRONCHOVIDEOSCOPE
OLYMPUS BF-H1100

BRONCHOVIDEOSCOPE
OLYMPUS BF-1TH1100
There are two new scopes available: the BF-H1100 and BF-1TH1100.
The BF-H1100 features a distal tip of just 4.9mm, while incorporating a large 2.2mm instrument channel. This provides plenty of room to insert any tool required – including a regular EBUS probe with a guide, needles, forceps and cryoprobes. It will also be possible to insert ablation technology when it becomes available.
At 5.8mm, the BF-1TH1100 has a larger outer diameter, but it also boasts a 3.0mm instrument channel. This oversized channel offers significant advantages, especially considering what’s coming next.
In the near future, new techniques will come into use – not for cancer, but for other diseases – that will require an instrument channel larger than the 2.8mm of the preceding model. Scopes with a normal outer diameter, but a bigger instrument channel, will be essential. The 3.0mm instrument channel of the BF-1TH1100 is not only helpful in daily endoscopy right now, it will be even more valuable in the future.
4-2. Advanced Suction Capability
With improved suction capacity and bigger instrument channels, these new scopes make it much easier to suction blood out of the central airways or from the peripheral part of the airways when the cryoprobe is inserted. For procedures where a clean in and out operation is not possible, the enhanced suction power of these scopes is a significant improvement, making it possible to perform procedures much more quickly.
This increase makes a noticeable difference, reducing procedure time significantly – especially if there is a bleeding problem. Regardless of whether blood or other residue is being removed from the lungs, the operation proceeds much more quickly thanks to the larger instrument channels.
5. EVIS X1 in Bronchoscopy
Together the new EVIS system and the new scope series offer endoscopists a powerful new tool for bronchoscopy. One touch activation of enhanced modes for more accurate observation in both near regions and far regions, as well deeper penetration into the mucosal layer, combined with sophisticated digital analysis and superior image quality assure better visualization of accessible areas and support more reliable diagnostic performance and improved therapeutic performance, marking the way forward in interventional pulmonology.
With a versatile array of features available at the press of a button, this new system eliminates the need for two units to cover all possible needs. Larger instrument channels make it safer from a patient perspective because blood and other debris can be removed as necessary to keep the site clean and maintain clear visualization. Ergonomic support such as the rotation function, the single cable and various other features are really helpful for the entire endoscopy team. With so many useful features, the launch of this new system marks the beginning of Olympus’s next success story.
Trademarks, product names, logos, or trade names used in this document are generally registered trademarks or trademarks of each company.
- Content Type