Fumihiro Asano, MD, PhD
Department of Pulmonary Medicine,
Gifu Prefectural General Medical Center
Disclaimer:
- TXI™, RDI™, and NBI™ Technologies are not intended to replace histopathological sampling as a means of diagnosis
- The positions and statements made herein by Dr. Asano, are based on Dr. Asano’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- The BF-1TH1200 used in this case is not available in the US market at this time nor is there an established time for its release. The safety and effectiveness of this product and or the use of these products has not yet been established in the United States market.
- The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
- Dr Asano, the authoring physician(s) of this presentation, are/ is a paid consultant(s) to Olympus Corporation
Scope: BF-1TH1200
Case:Right lung tumor
Location: Between the right intermediate trunk and the right upper lobe bronchus
Patient information: Female, 70 years old
Medical history:While she was receiving treatment for emphysema at a local clinic, chest X-ray revealed a right lung mass and pleural effusion. She was then referred to our institution.
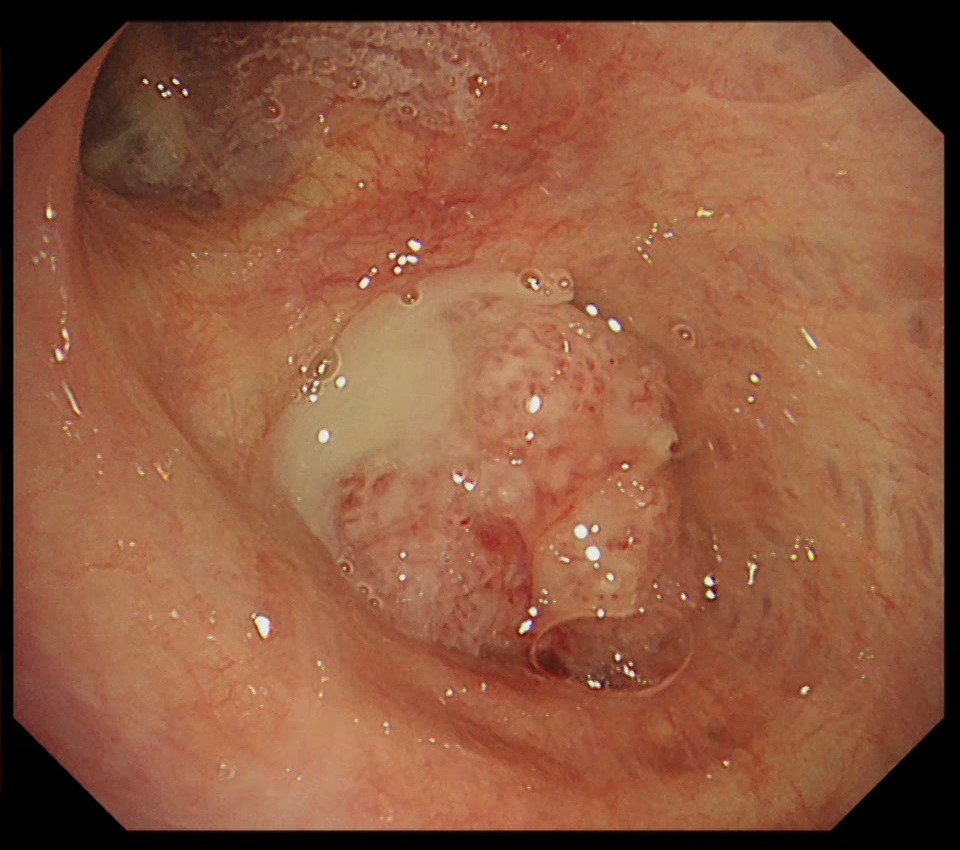
1. Tumor in the right intermediate trunk
(WLI)
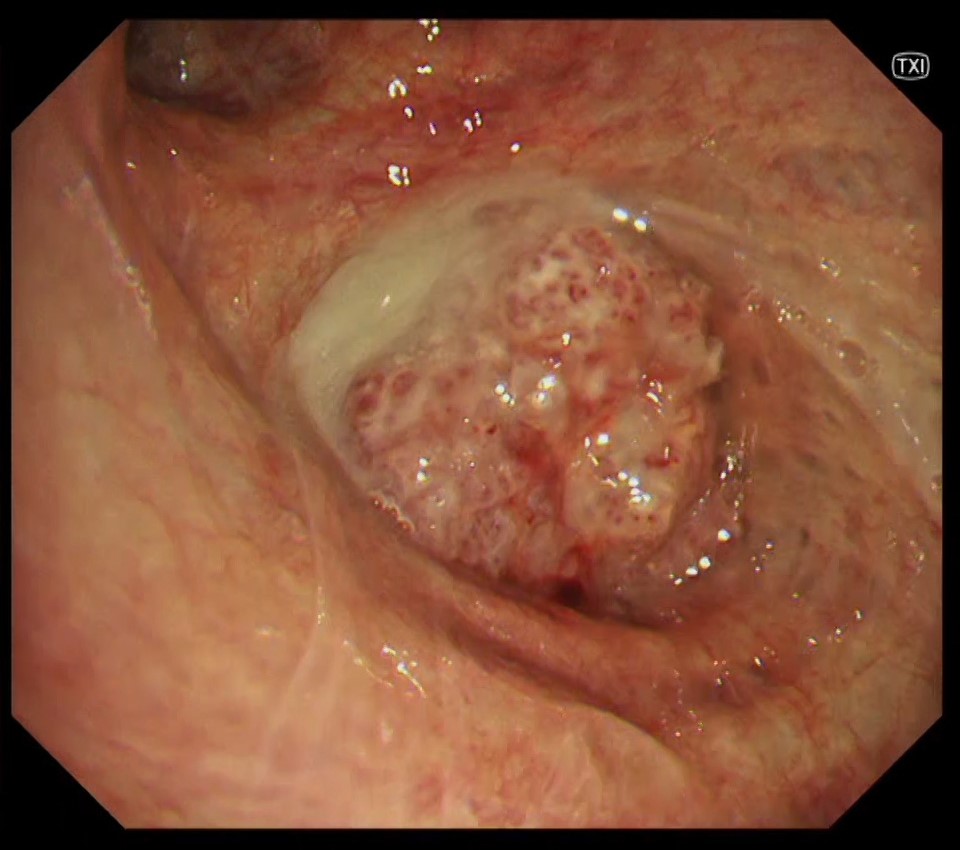
2. Tumor in the right intermediate trunk
(TXI™ Technology)
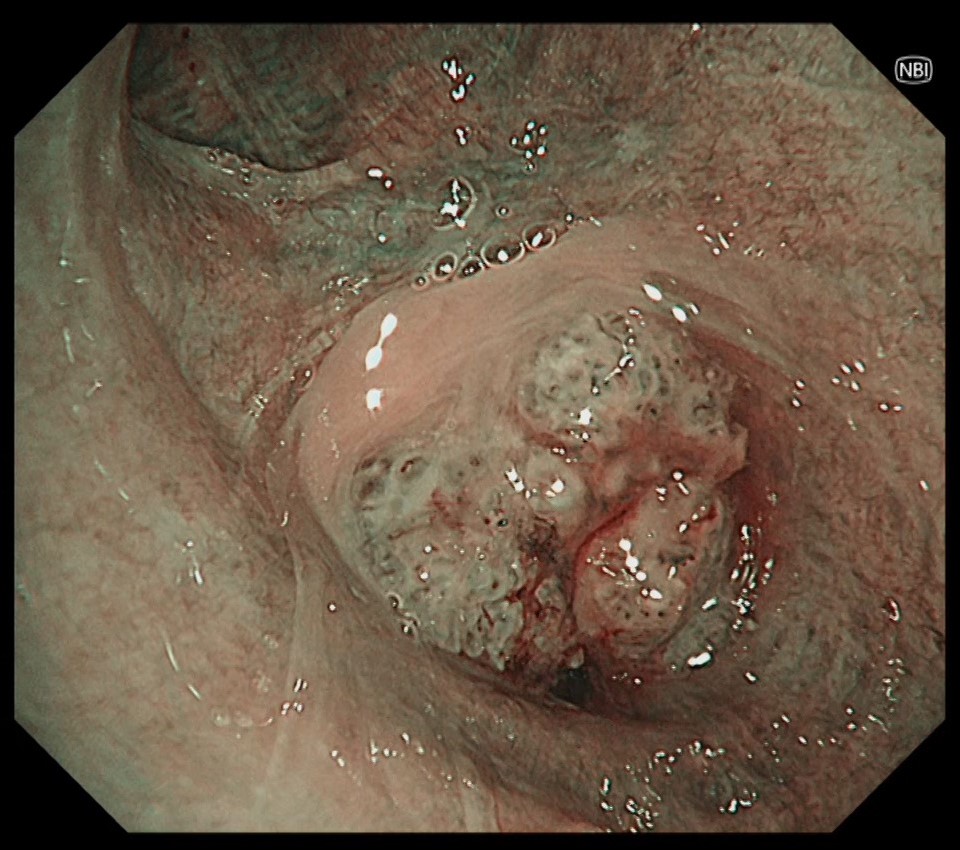
3. Tumor in the right intermediate trunk
(NBI™ Technology)
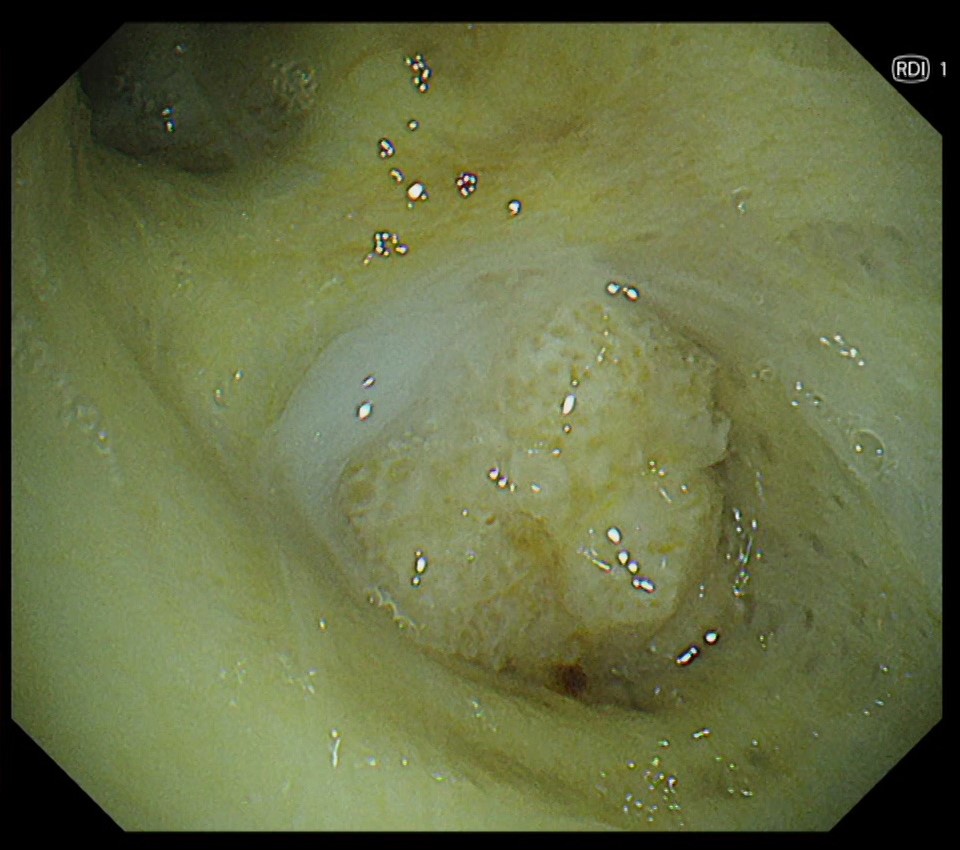
4. Tumor in the right intermediate trunk
(RDI™ Technology)
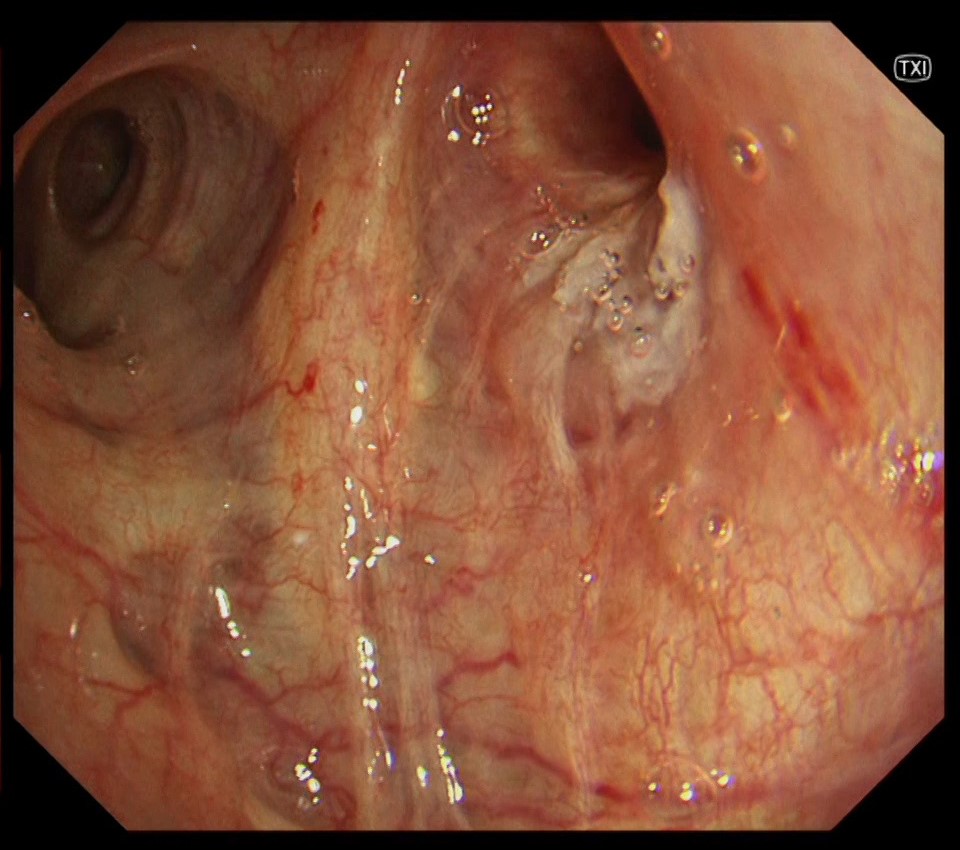
5. Lesion in the right upper lobe bronchus
(WLI)
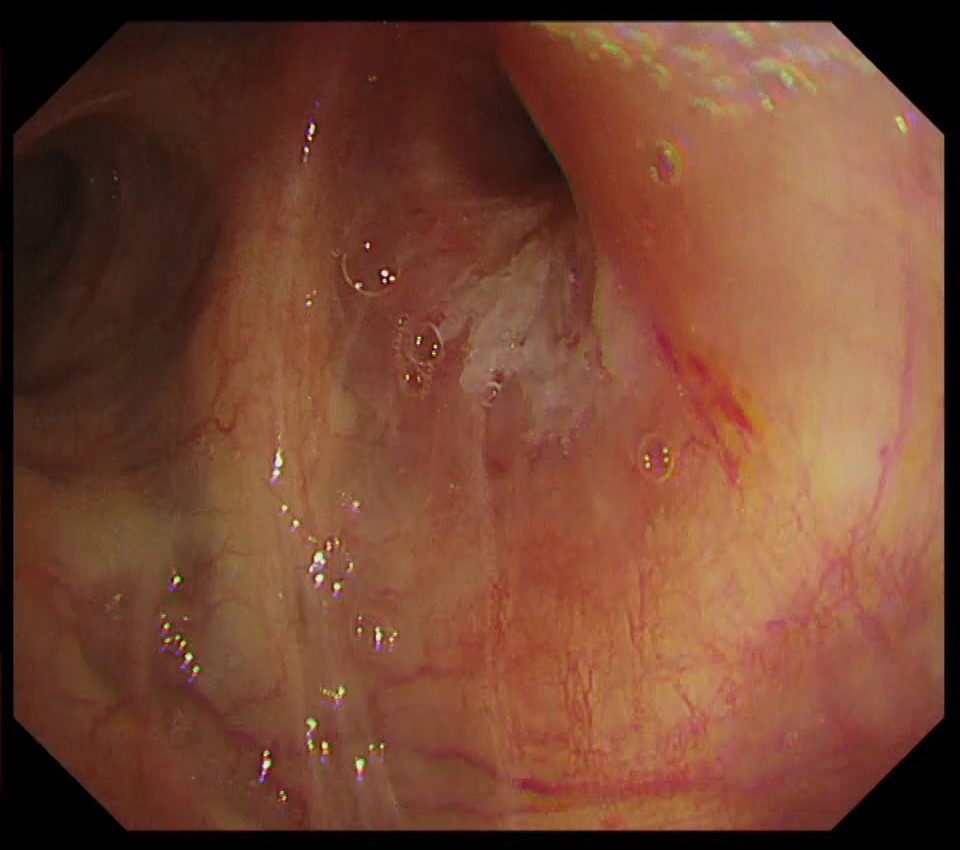
6. Lesion in the right upper lobe bronchus
(TXI™ Technology)
Case Video
Pathological Findings
- The tumor located in the intermediate trunk was biopsied endoscopically and diagnosed as squamous cell carcinoma with keratinization.
- The tumor cells tested positive for p40 but negative for TTF-1.
Overall Comment
This case is a lung squamous cell carcinoma originating from beyond the intermediate bronchus, with suspected infiltration into the upper lobe bronchus wall from lymph node metastasis in the hilum. TXI™ technology has the advantage of observing not only abnormal findings such as red dots and bridging fold, but also the intricate vascular network of normal areas in greater detail compared to WLI. This makes it easier to comprehend the extent of the lesion’s infiltration.
- Content Type