VOLUME REDUCTION OF HYPERTROPHIC TONSILS
In the following chapter, it is demonstrated how to use bipolar radiofrequency-induced thermotherapy (RFITT) to reduce the volume of hypertrophic tonsils in children.
01 | Anesthesia and Medications
This procedure is commonly performed on children aged three and over in an operating room. In children from year three to eight, it is recommended to use intubation anesthesia. In older children, however, a laryngeal mask can be used to administer anesthesia.
In adults, tonsils can be treated with bipolar radiofrequency-induced thermotherapy using local anesthesia. First, use, for example lidocaine pump spray for superficial anesthesia of the tongue and the pharynx. Then apply local anesthesia to the mucous membrane of the anterior and posterior palatine arches and the peritonsillar tissue with approximately 10 ml of one percent lidocaine solution with epinephrine 1 : 200,000.
Perioperative antibiotic prophylaxis, for example cephalosporin, is rarely necessary.
02 | Treatment of the Tonsils (with RFITT)
Power settings: A power setting of 7 watts (mode: PureRFITT) is recommended to make lesions in large palatine tonsils. The power setting on your control unit determines the extent of coagulation induction. The lower the power setting, the longer the application time and the greater the extent of coagulation. The higher the power setting, the smaller the area of the coagulation.
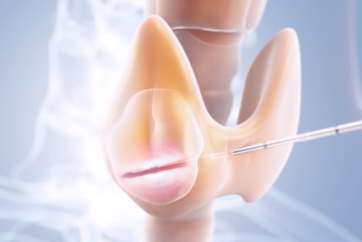
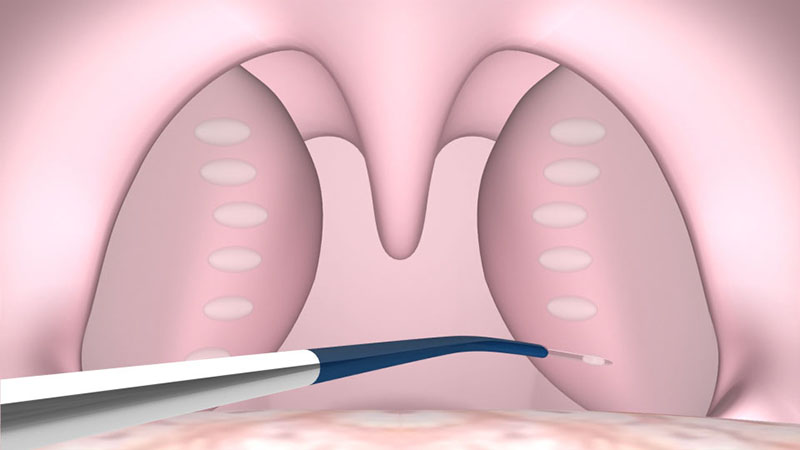
Use the CelonProSleep plus applicator to treat hypertrophic tonsils.
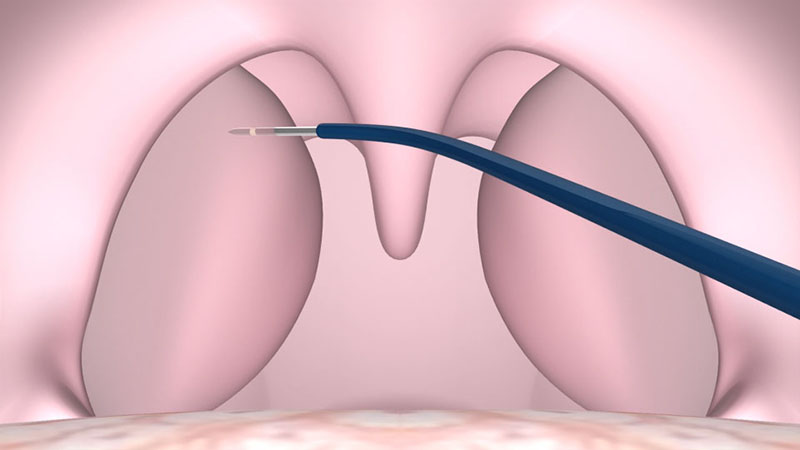
Insert the applicator into the tonsils until the insulating tube of the probe touches the tissue [Figure 01a/b].
After positioning the probe, activate the power supply by pressing the foot switch. You can monitor the status of coagulation via the acoustic signal. The power supply is reduced automatically to prevent overdose effects.
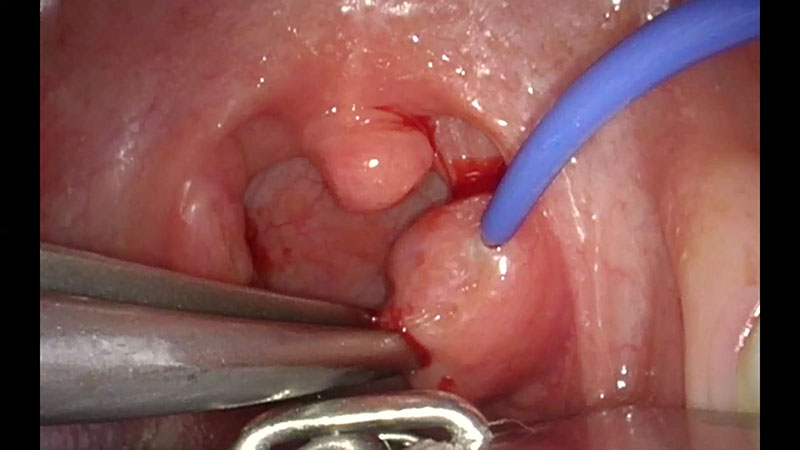
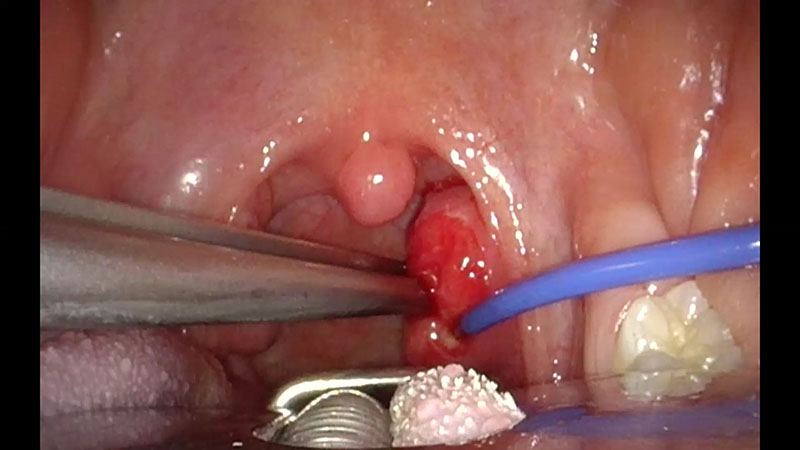
It is recommended to separate the points of insertion by approximately 1 cm. The number of insertions required depends on the size of the tonsils, but usually involves four to six punctures [Figure 02a/b].
Note:
- Take care not to penetrate the underlying tonsil capsule.
- During the coagulation process, avoid the immediate area of the tonsil bed by pulling the tonsils away from the critical structures and towards the median plane [Figure 01b].
A little blanching may occur, which is normal and not a reason to stop the coagulation.
Due to the soft lymphatic tissue of children, the application takes up to ten seconds for each lesion. It might be necessary to clean the tip between coagulations.
Bleeding is rare, and in most cases soon stops on its own.
03 | Therapeutic Treatment
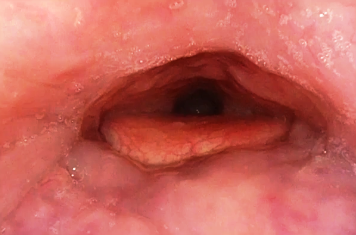
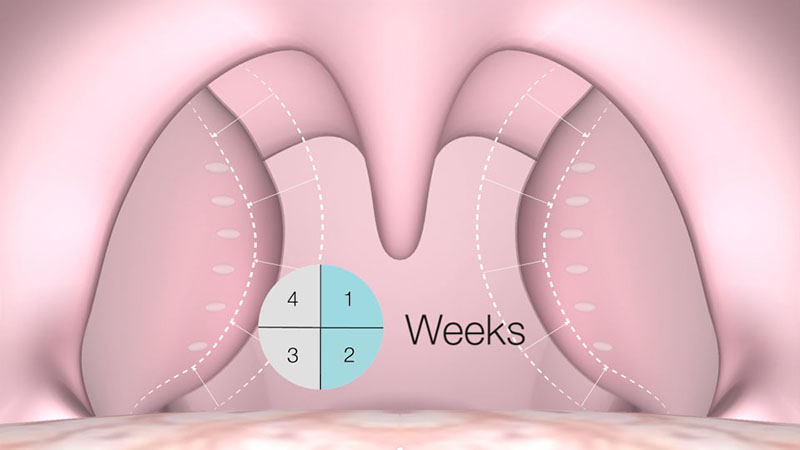
The coagulated tissue is absorbed over the next three to four weeks by the body’s own absorption process, leading to a volume reduction of 30 to 40 percent [Figure 03a/b].

04 | Postoperative Care
Because of the risk of swelling, it is recommended to keep children under postoperative observation for at least a couple of hours after the procedure. Adults can go home straight after the procedure.
For postoperative pain treatment, ibuprofen or paracetamol are recommended for children, and diclofenac is recommended for adults. A follow-up visit should be scheduled for the next morning, then again after three weeks.
Treatment with the CELON method can be repeated without any problems six weeks later, if required.
Note:
- This procedure should not be performed on children under three.
- If your patient has chronically recurrent tonsillitis, thermo-therapeutic treatment is not recommended.
- This procedure should also not be used to treat ‘kissing tonsils’ in small children due to the risk of postoperative swelling.
- Content Type