
Anna Wiechowska-Kozłowska
MD, PhD
Introduction
In the era of development of excellent imaging modalities, such as multi-slice computed tomography and magnetic resonance imaging, endoscopic ultrasound examination has its unique importance, as it allows not only to visualize lesions difficult to evaluate in other examinations, but also to collect material for microscopic examination. Thanks to the different diameter and construction of needles, it is possible to obtain both cellular material for cytological examination and tissue material – for histopathological examination. The choice of the type and diameter of the needle depends on the size of the lesion, its location, nature, but also on the individual assessment of the endoscopist performing the examination and the pathomorphologist cooperating with him. The most important rule in needle selection is that the biopsy result should allow unambiguous diagnosis of the disease and the safest possible procedure.
EUS-FNA biopsy
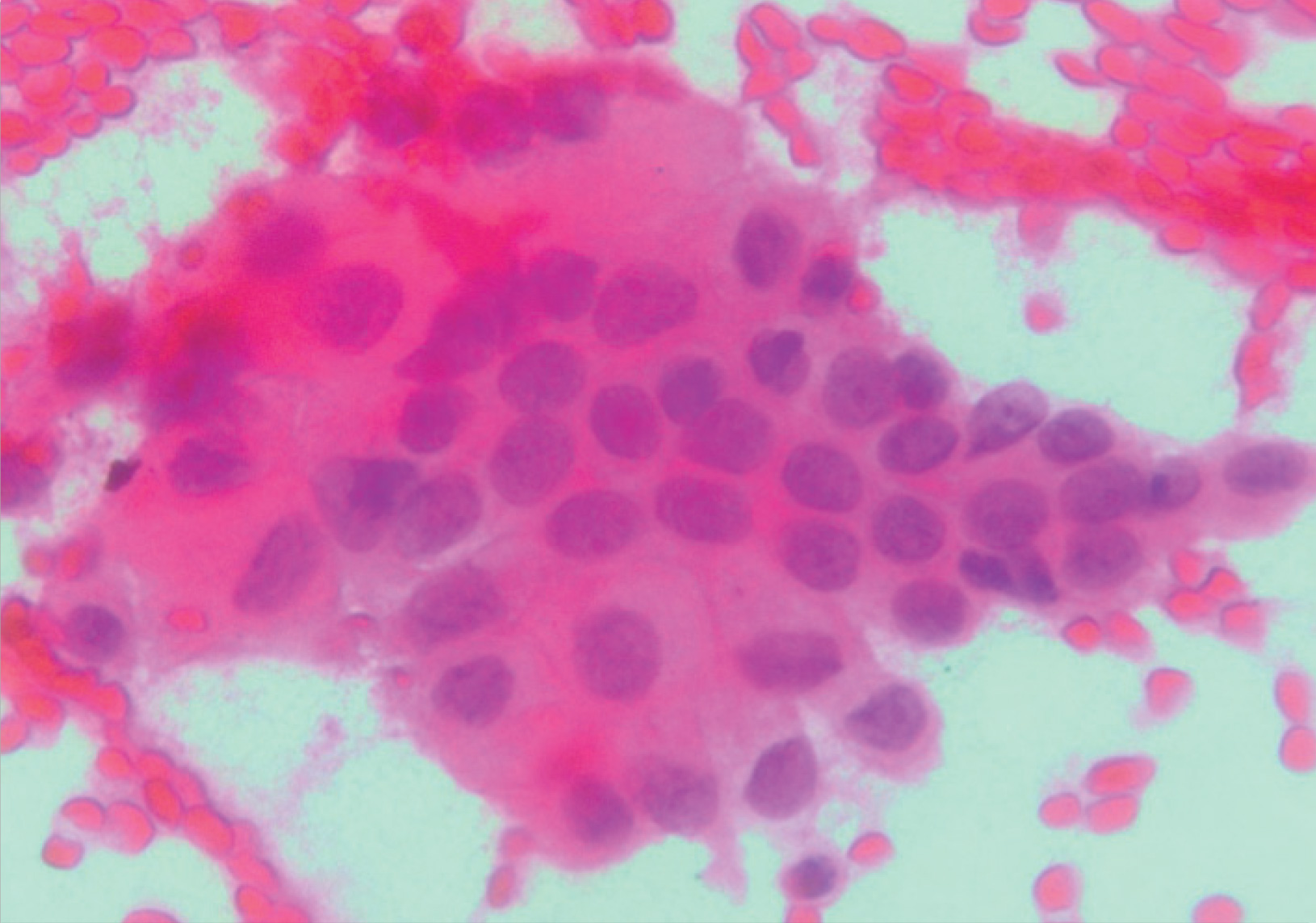
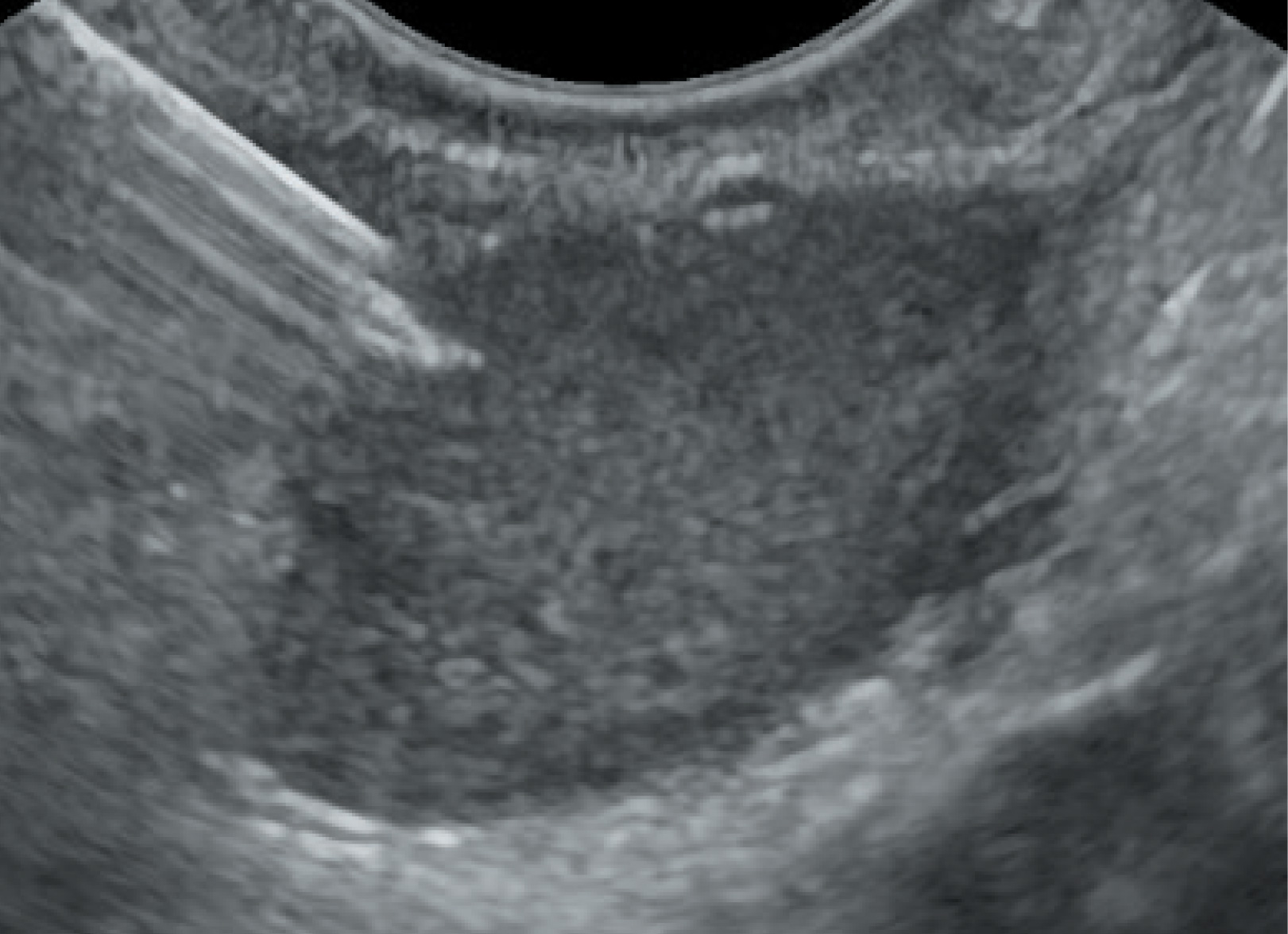
Classic fine needle aspiration biopsy needles allow the collection of cell-cytological material (EUS-FNA). The accuracy of the cell-cytological material collection (EUS-FNA) and have been used for years in the puncture of lesions suspected of having cancer cells. Biopsy of focal lesions, confirming the presence of cancer cells of the pancreas (Fig. 1), gastric wall, focal lesions of the liver or biliary tract determines the further management and decides on the choice of treatment. Standard Olympus 22G needles have been widely used in these indications for years.
In selected cases, they can be replaced by needles with a smaller diameter, i.e. 25G. Based on years of experience and data from the literature, it seems that the main indications for their use are:
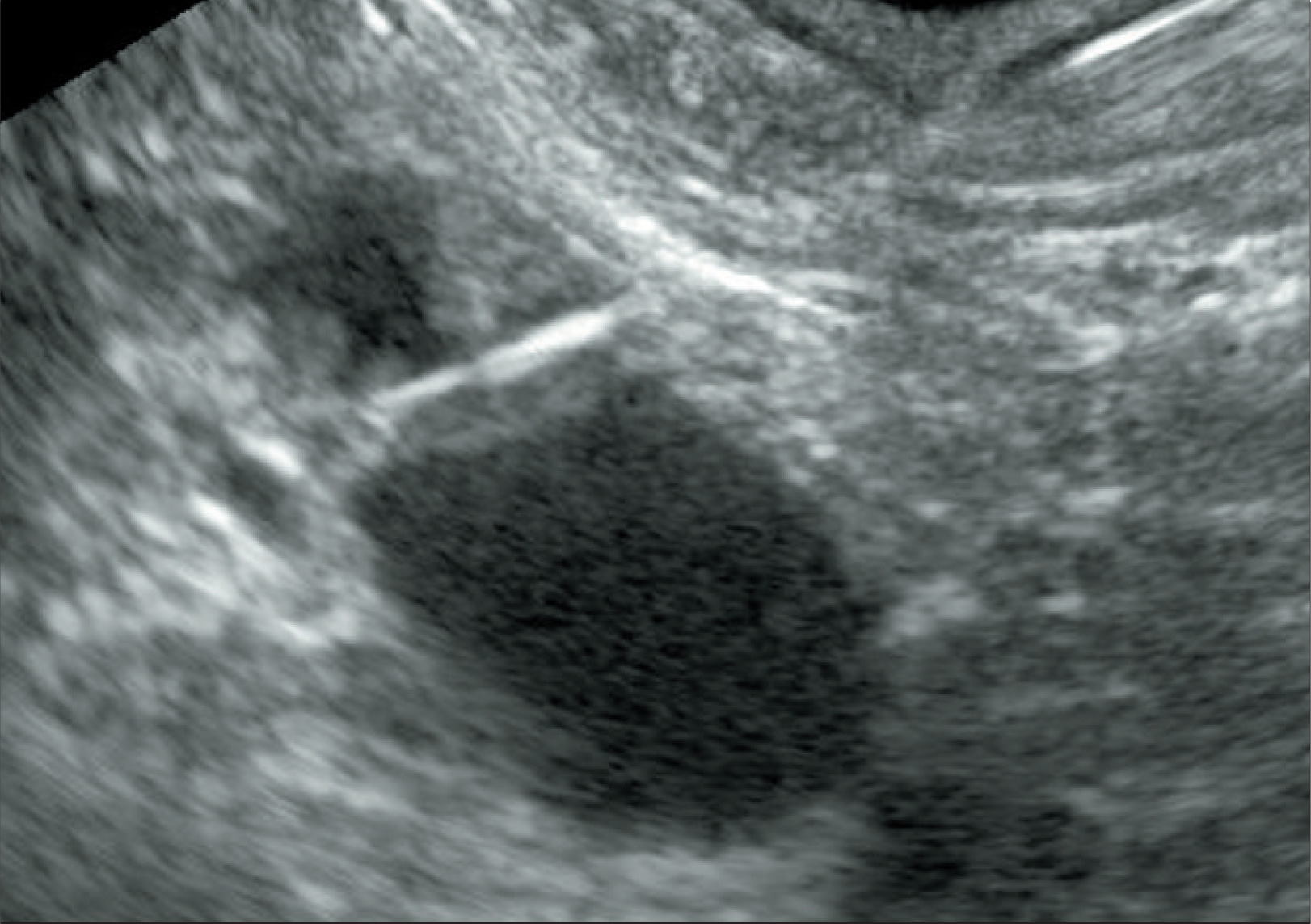
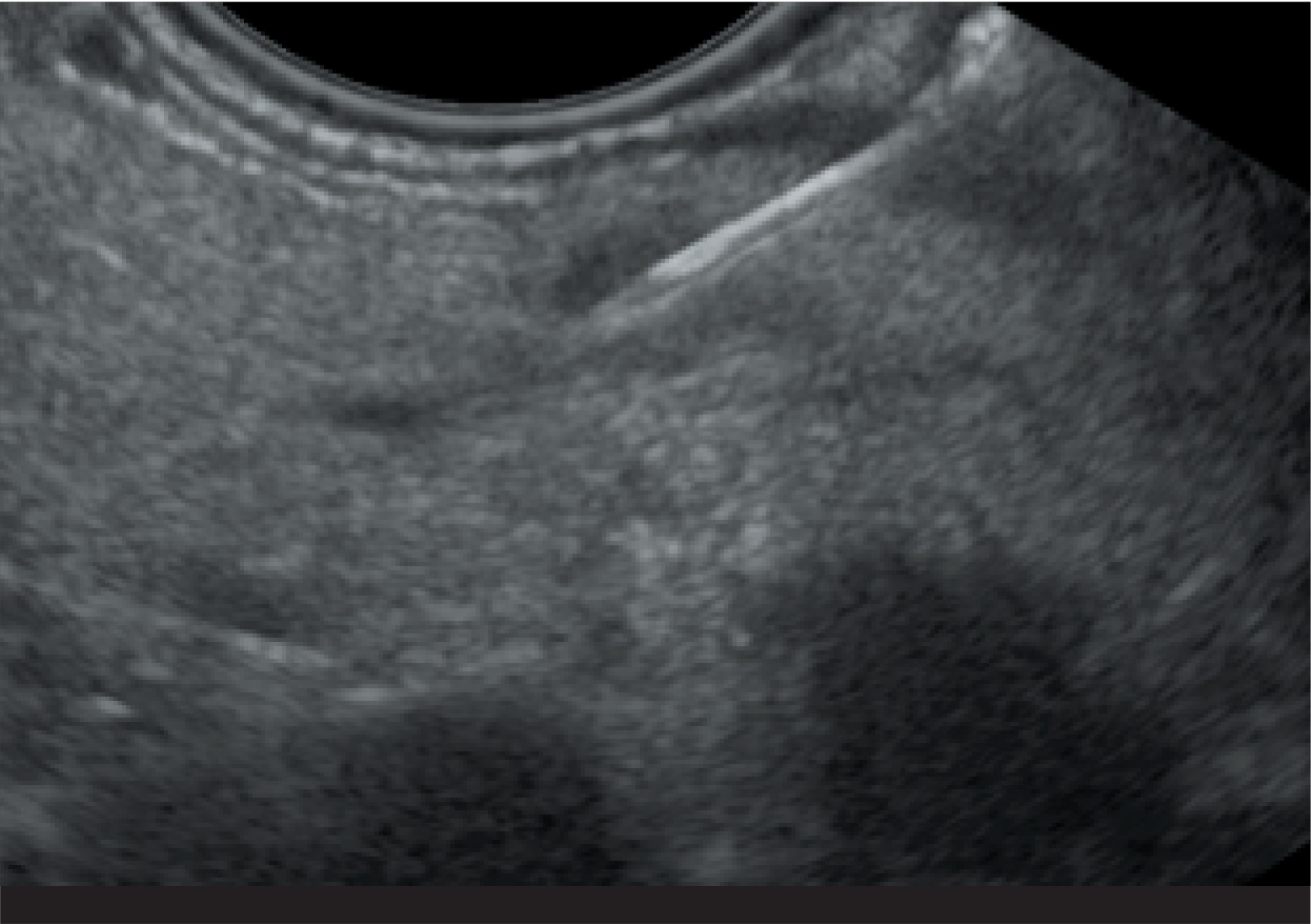
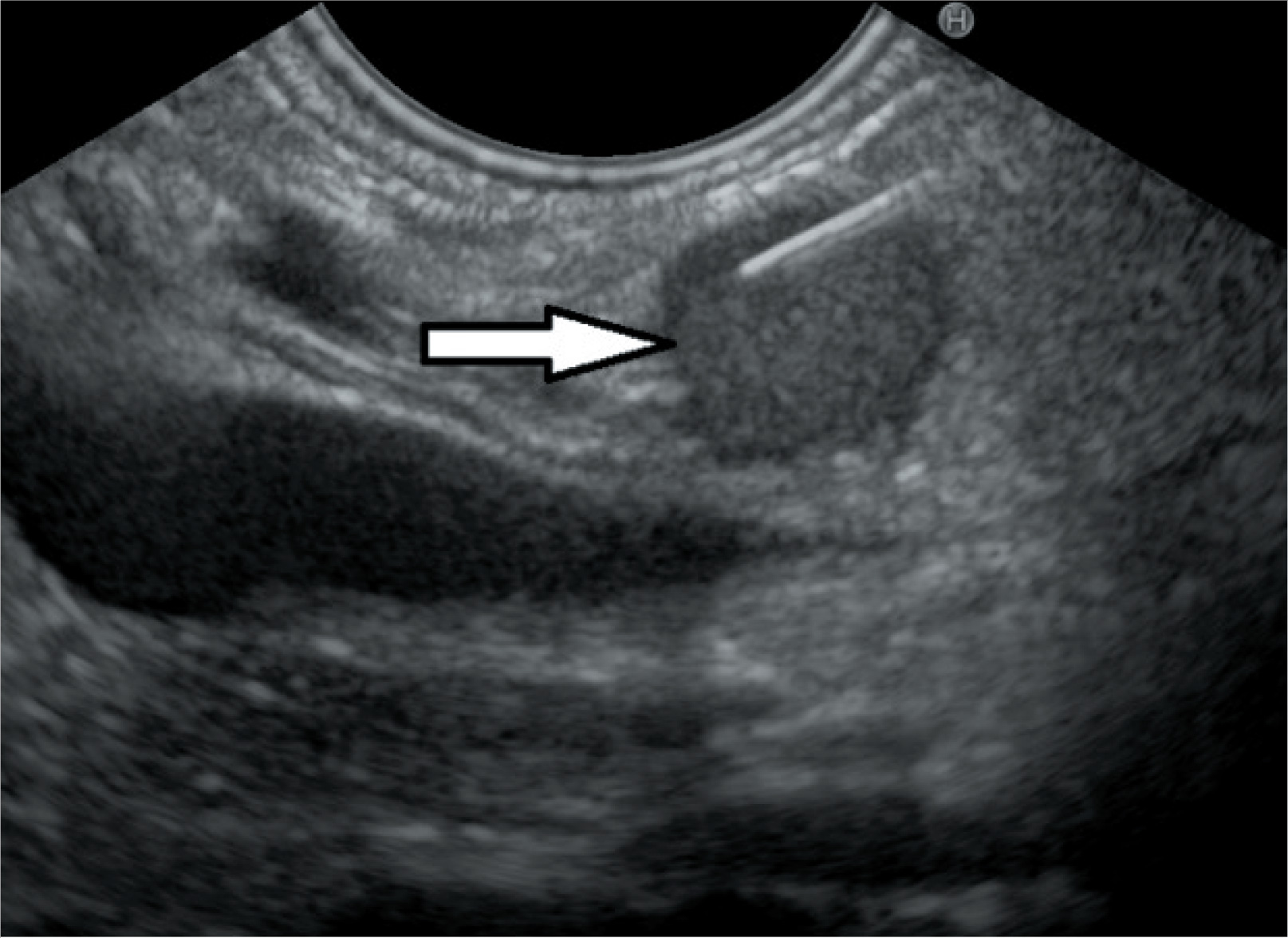
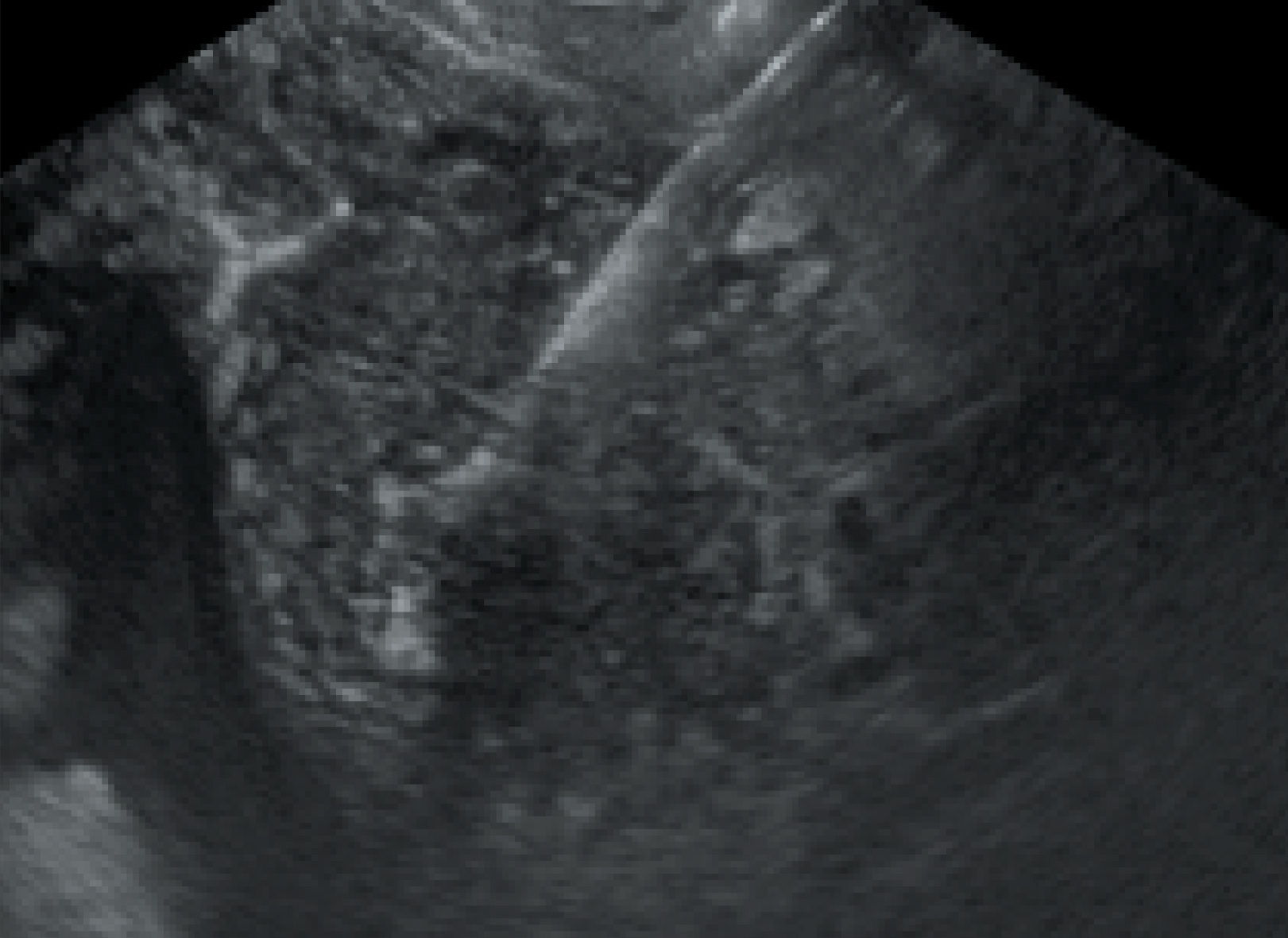
- very small size of the lesion, qualified for biopsy – small focal lesions of the pancreas or liver with a diameter of about 5 mm (Fig. 2.2)
- nodules adjacent to cystic lesions (Fig. 2.1)
- focal lesions, difficult to puncture
EUS-FNB biopsy
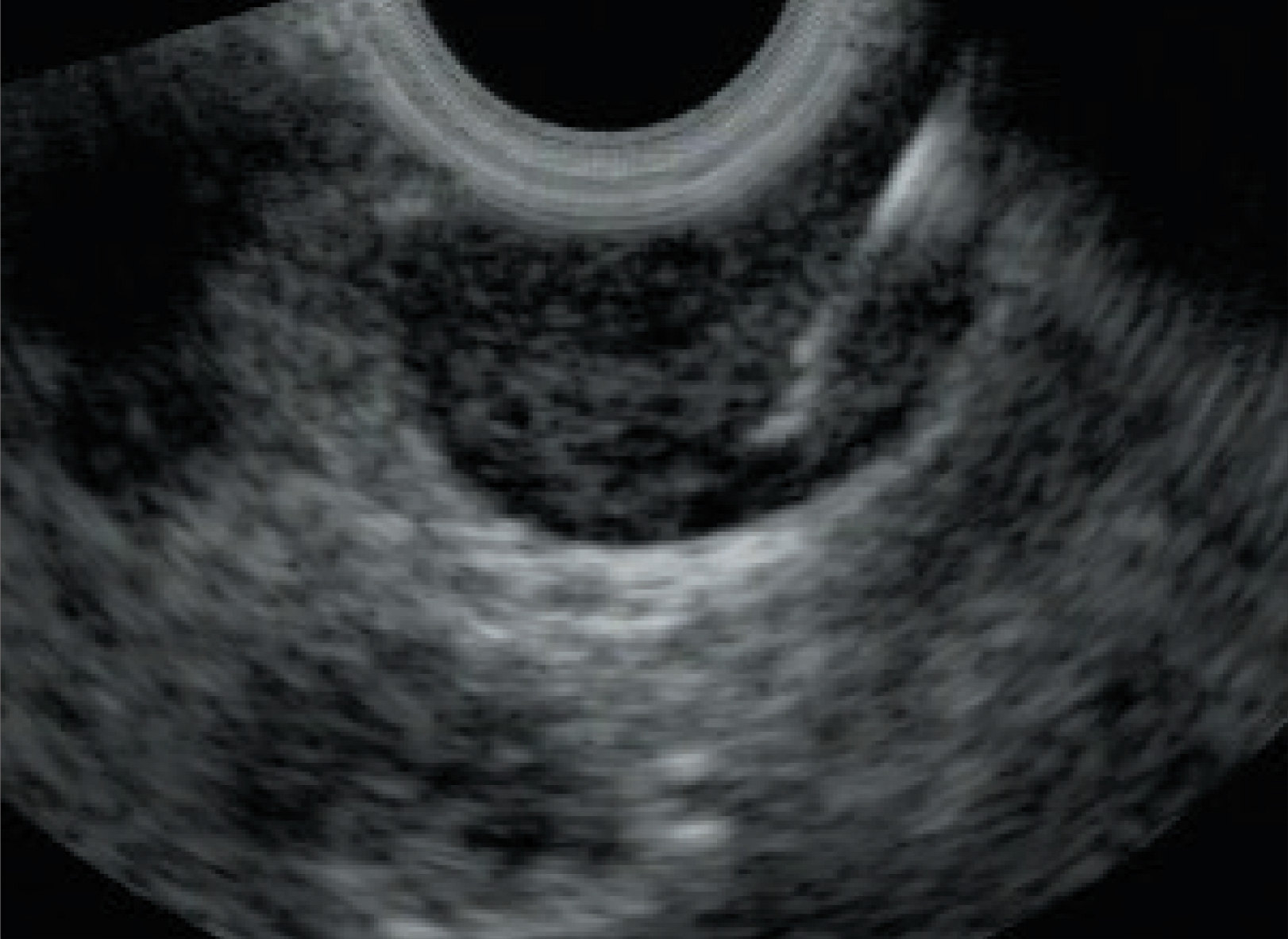
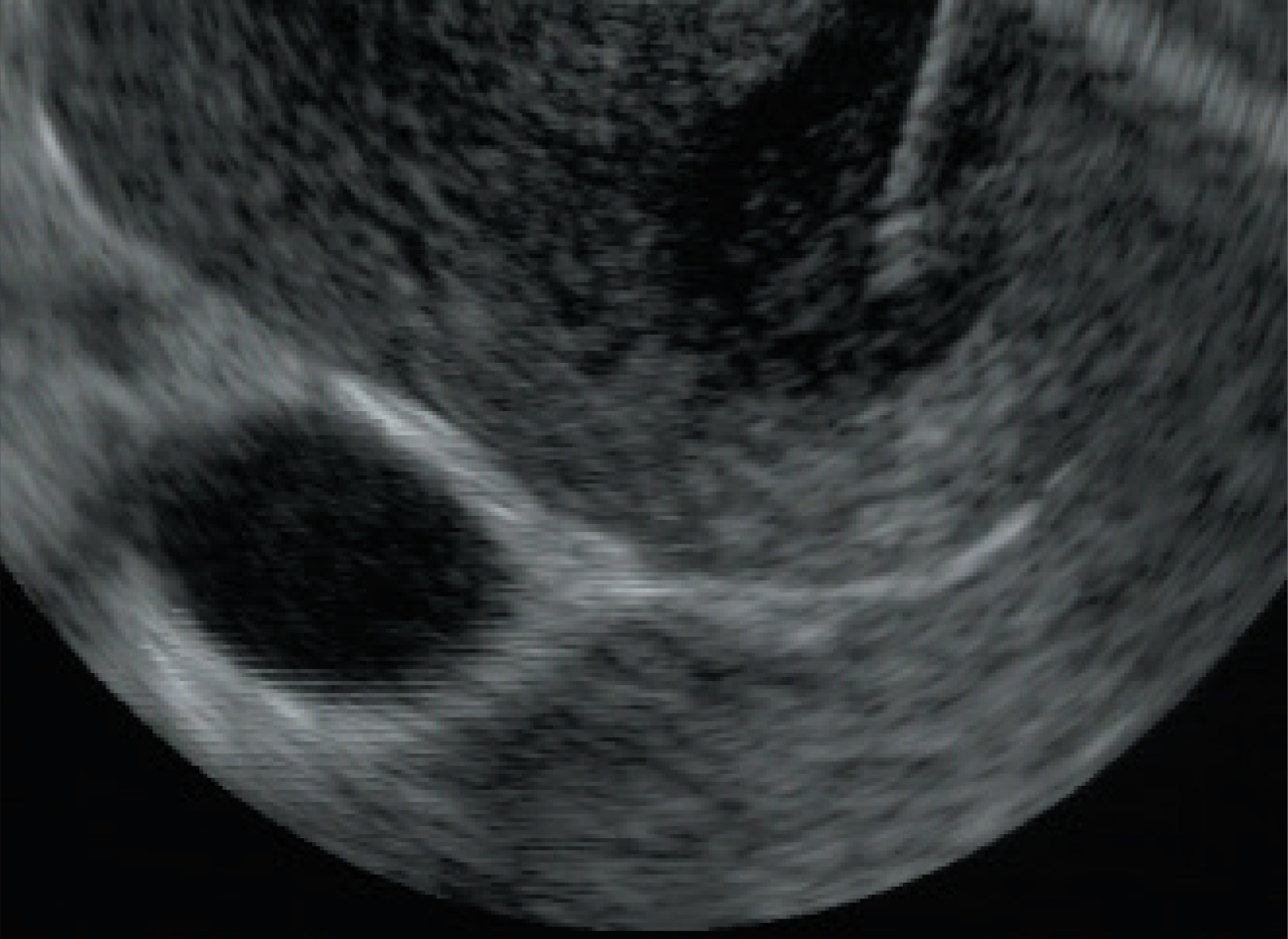
Thanks to modern technologies it is possible to perform fine needle biopsy with taking a sample of tissue for histopathological examination, so called EUS-FNB biopsy (Fig. 4a & 4b). EZ Shot 3 Plus needles
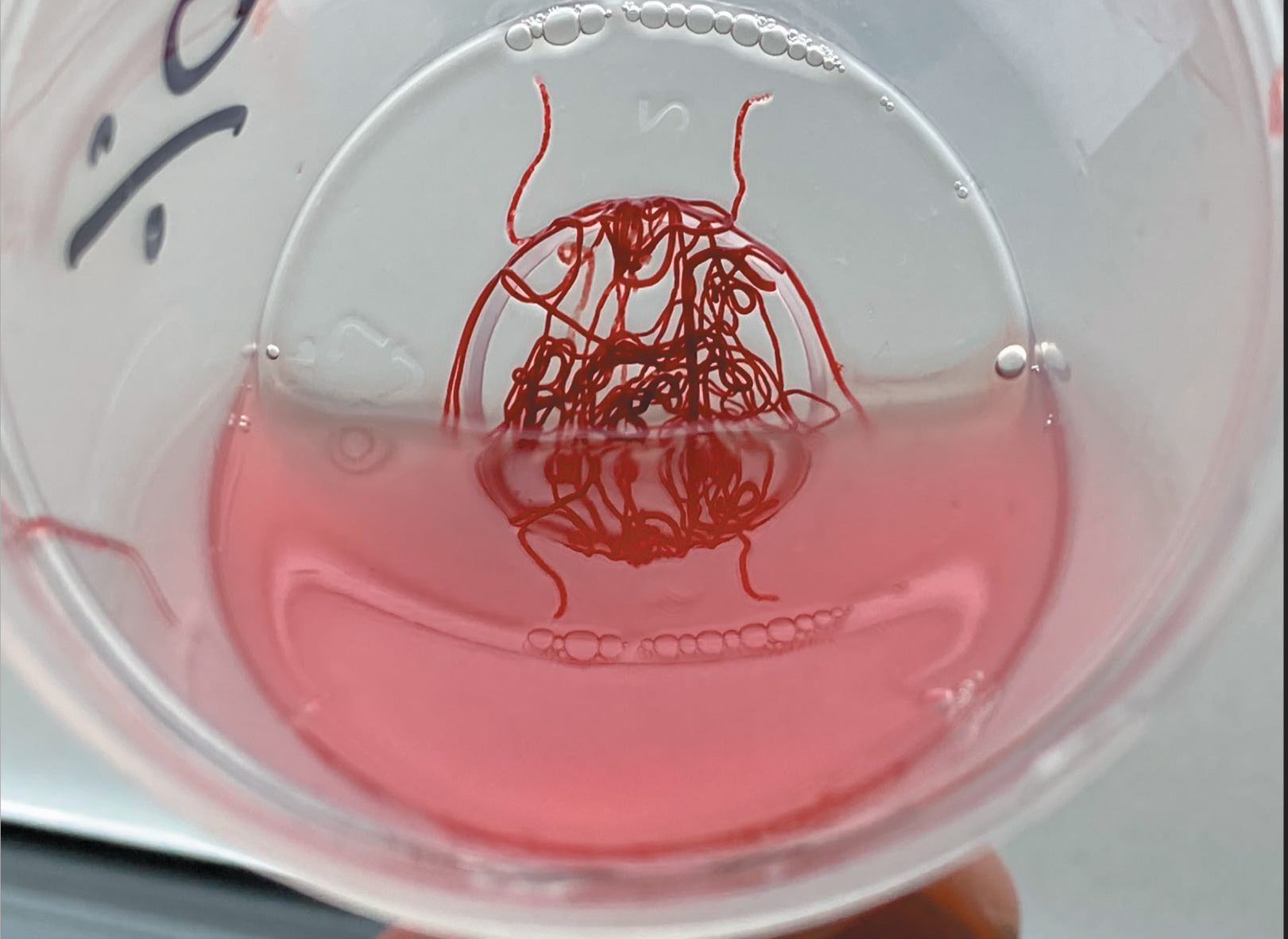

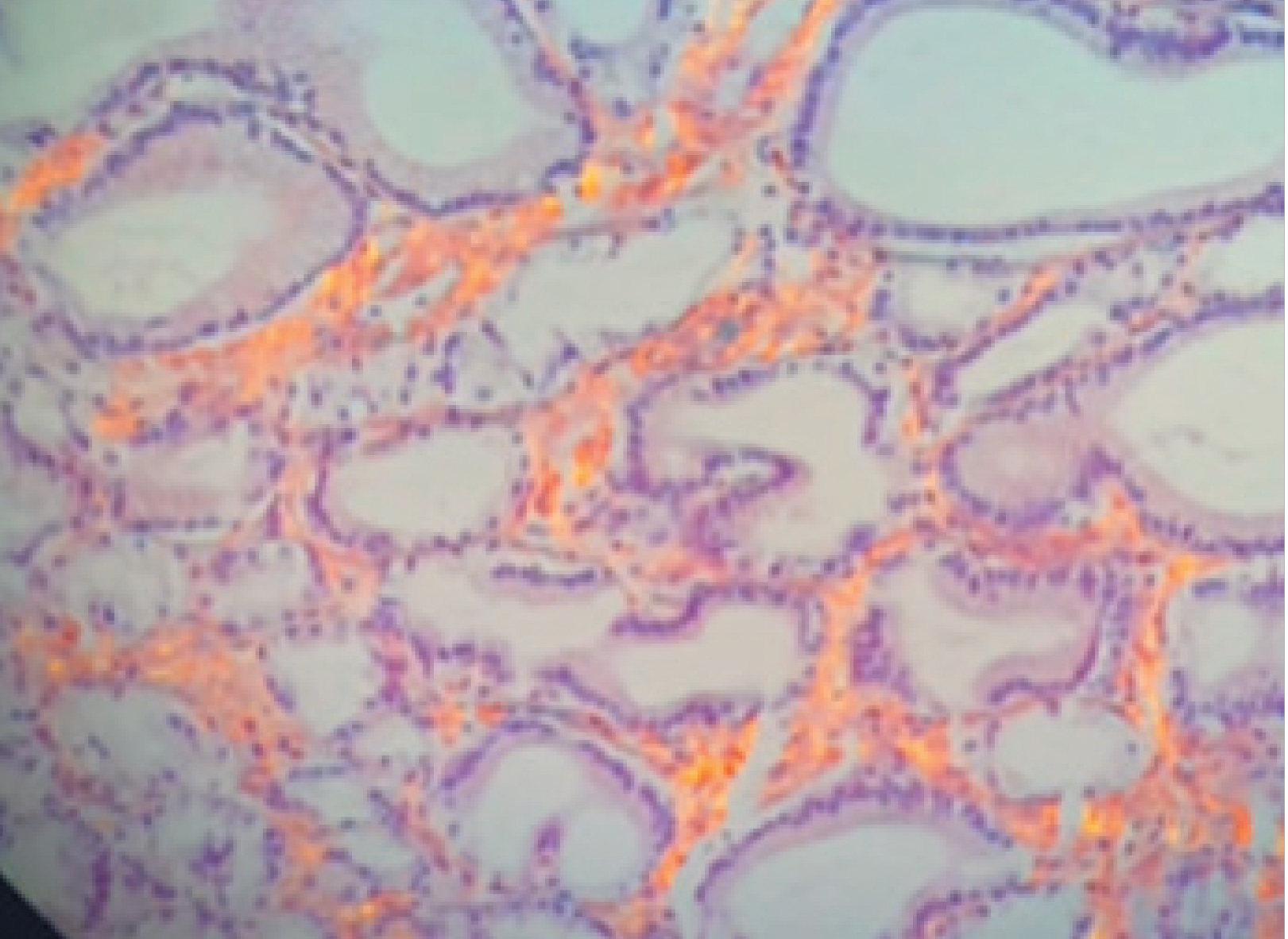
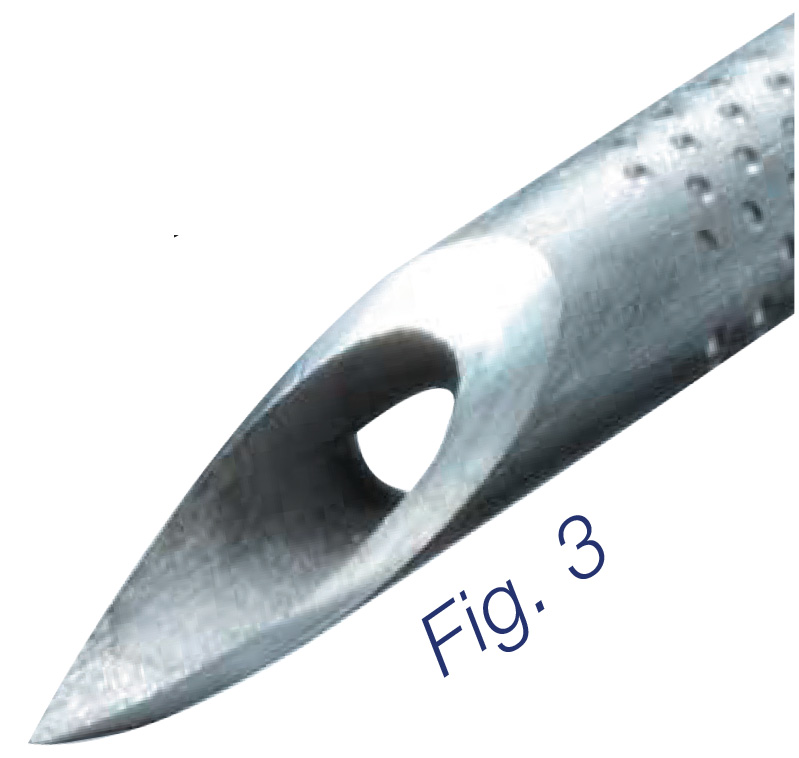
22G and 25G, thanks to their special construction – Menghini cut (Fig. 3) – allow not only to establish the diagnosis of malignant neoplasm, but also provide a number of other possibilities, e.g. determination of type or degree of malignancy, which is possible only on the basis of immunohistochemical and other molecular tests (Fig. 5).
- pancreatic neuroendocrine tumours (PNETs) (Fig. 6.1)
- gastric stromal tumours (GIST) and their differentiation with other submucosal tumours (Fig. 6.2)
- autoimmune pancreatitis (Fig 6.3)
- lymph nodes (Fig. 6.4), but also – pancreatic cancer with the possibility of a deeper assessment of the nature of the lesion, including satellite instability (Fig. 6.5)
- focal and parenchymal liver lesions (Fig. 6.6)
- thickened gastric wall

Conclusions
The EZ Shot 3 Plus biopsy needles, thanks to the special cut of the blade, typical for classical fine needles, allow relatively easy insertion of the needle into the focal lesion, without any resistance during insertion or bending on its surface. This type of blade, thanks to its minimal diameter, also ensures the greatest safety of puncture, corresponding to classical fine needles. At the same time, EZ Shot 3 Plus needles, thanks to the construction, allow to take a tissue samples previously obtained only through thick-needle biopsies. This ease of puncture, good needle imaging and high safety with simultaneous possibility of obtaining a large tissue fragment are decisive for the unique capabilities of EUS biopsies with EZ Shot 3Plus. They combine the ease and safety of a typical fine-needle puncture with the acquisition of histopathological material, with far greater specificity and sensitivity for diagnosing the nature of the lesion.
Author
Anna Wiechowska-Kozłowska, MD, PhD, since 2007 the Head of the Endosonography Unit at the Central Clinical Hospital of the Ministry of Internal Affairs & Administration in Szczecin, for 14 years has performed annually approx. 400 biopsies under EUS guidance.
- Keyword
- Content Type




