EXTRACORPOREAL SUTURING
Pushed half knot
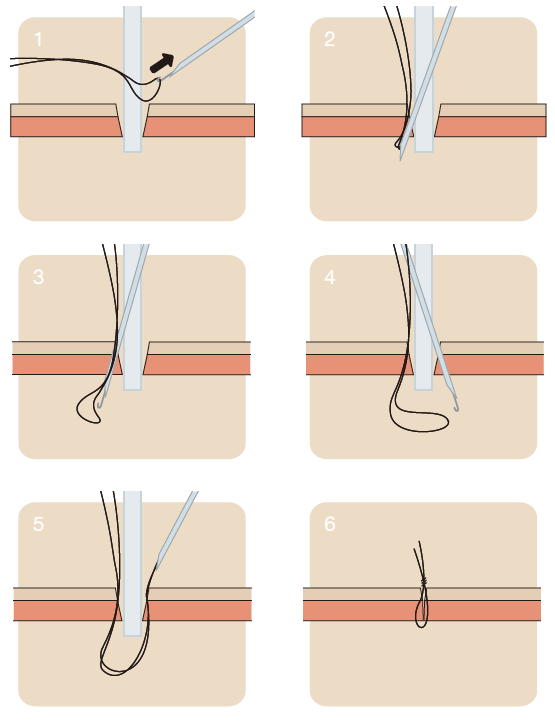
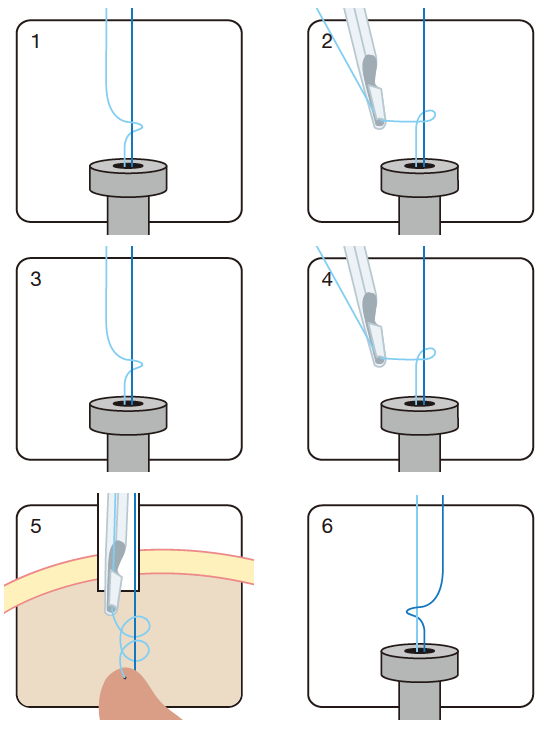
Extracorporeal pushed half knots can be a good alternative to the more difficult to perform extracorporeal knots. They derive from classical surgery and most surgeons are familiar with this type of knot.
The suture is pushed through the trocar and the needle is stitched through the tissue. Then the suture is positioned back to the patient’s exterior via the same trocar route. One end of the suture is held under light tension. A first half knot is tied (figure 1).
By using the knot pusher this half knot is pushed downwards (figure 2 and 3).
Another half knot is performed in the same way (figure 4), pushed down and tightened (figure 5).
A final third half knot (figure 6), tied in the opposite, is pushed down fixing the knot.
The arrangement of the first and the second half knot, both tied in the same way and the final third knot, which is tied in opposite direction, will fix the knot.
Roeder knot
Performing Roeder knots (or other knot techniques such as Melzer/Bueß or Weston knot) requires certain skills. The application of a preformed Roeder loop integrated into a plastic pusher device is easier.
The Roeder sling technique can be thought of as a lasso technique which can be tightened only in one direction. Clinical application is primarily to ligate tissue, e.g. vessels or the appendix.
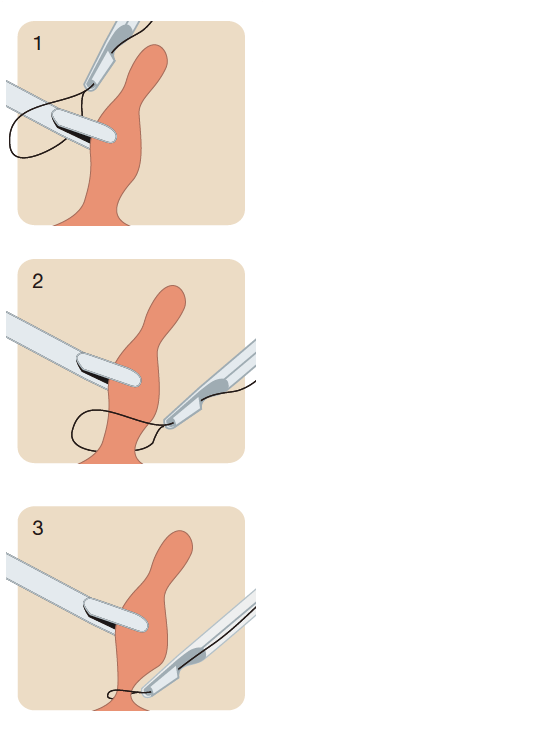
A grasping instrument is placed through the loop and grasps the tissue. The loop is pushed, tightened and closed and ligates the tissue very effectively.
As the preformed Roeder loop is suitable for appendix surgery, the knot preparation done by the surgeon allows the application in almost every indication for ligation. After the tissue penetration is completed and the suture is positioned back to the exterior of the body, the Roeder knot is performed manually.
The knot is pushed down to the tissue again with a specially designed knot pusher. The tissue will adapt by pulling the suture and finally the ligation is completed.
Roeder knot
Fascial closure
Trocar site herniation is a recognized complication in laparoscopic surgery. The recommendation to close a trocar incision by suturing depends mainly on the diameter of the trocars used.
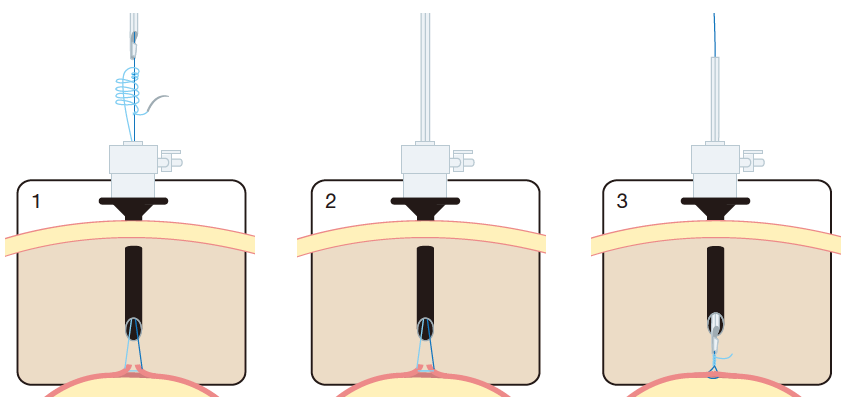
One common technique to close the fascia is to use a fascial closure needle. It consists of a cannula with an
internal hook that can be retracted and extended. The suture is first placed around the hook outside the body. The hook with the attached suture is then retracted inside the cannula (figure 1).
This prevents dislocation of the suture when the cannula is inserted through the abdominal wall (figure 2).
Having passed the abdominal wall, the suture is released from the hook (figure 3) and the facial closure needle is withdrawn from the patient. In the next step, the “empty” needle is reinserted on the opposite side of the trocar through the abdominal wall (figure 4).
The suture is grasped with the needle’s hook and both the fascial closure needle and the suture are withdrawn from the abdominal wall. Finally the trocar itself is withdrawn (figure 5) and the suture is tied (figure 6). This way a safe and effective trocar closure can be achieved.