Author: Daisuke Himeji, MD, PhD
Miyazaki Prefectural Miyazaki Hospital, Japan
Endoscopy Center, Department of Internal Medicine, Department of Medical Informatics
Disclaimer:
- TXI™, NBI™, and RDI™ Technologies are not intended to replace histopathological sampling as a means of diagnosis
- The positions and statements made herein by Dr. Himeji’s are based on Dr. Himeji’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- The BF-H1200 used in this case is not available in the US market at this time nor is there an established time for its release. The safety and effectiveness of this product and or the use of these products has not yet been established in the United States market.
- The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
- Dr Himeji, the authoring physician(s) of this presentation, are/ is a paid consultant(s) to Olympus Corporation.
Scope: BF-H1200
Patient information: Female in her 70s
Medical history:
She consulted a local doctor after suffering from exertional dyspnea and wheezing that had continued for 3 months. A chest CT showed a mass compressing the airway in the left S6. Bronchoscopy was performed and squamous cell carcinoma was diagnosed. The patient was referred to us for surgery, and we performed bronchoscopy to assess the feasibility of surgery.
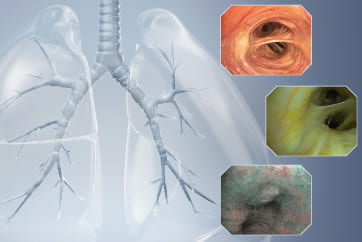
1. Whole image of the left lower lobe cancer (WLI)
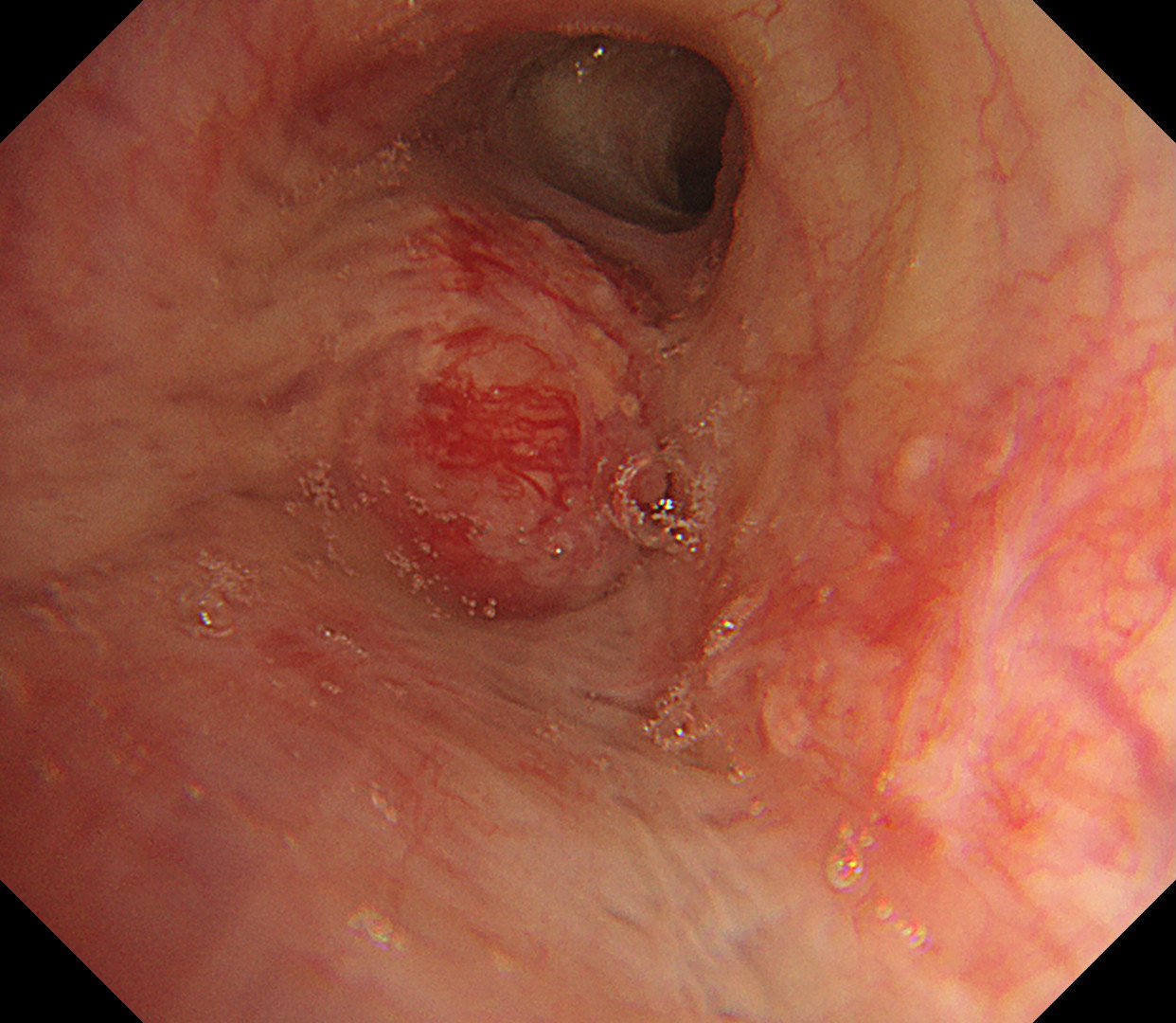
A tumorous lesion that blocks the entrance to the left lower lobe is recognized under white light imaging.
2. Whole image of the left lower lobe cancer (TXI™ Technology)
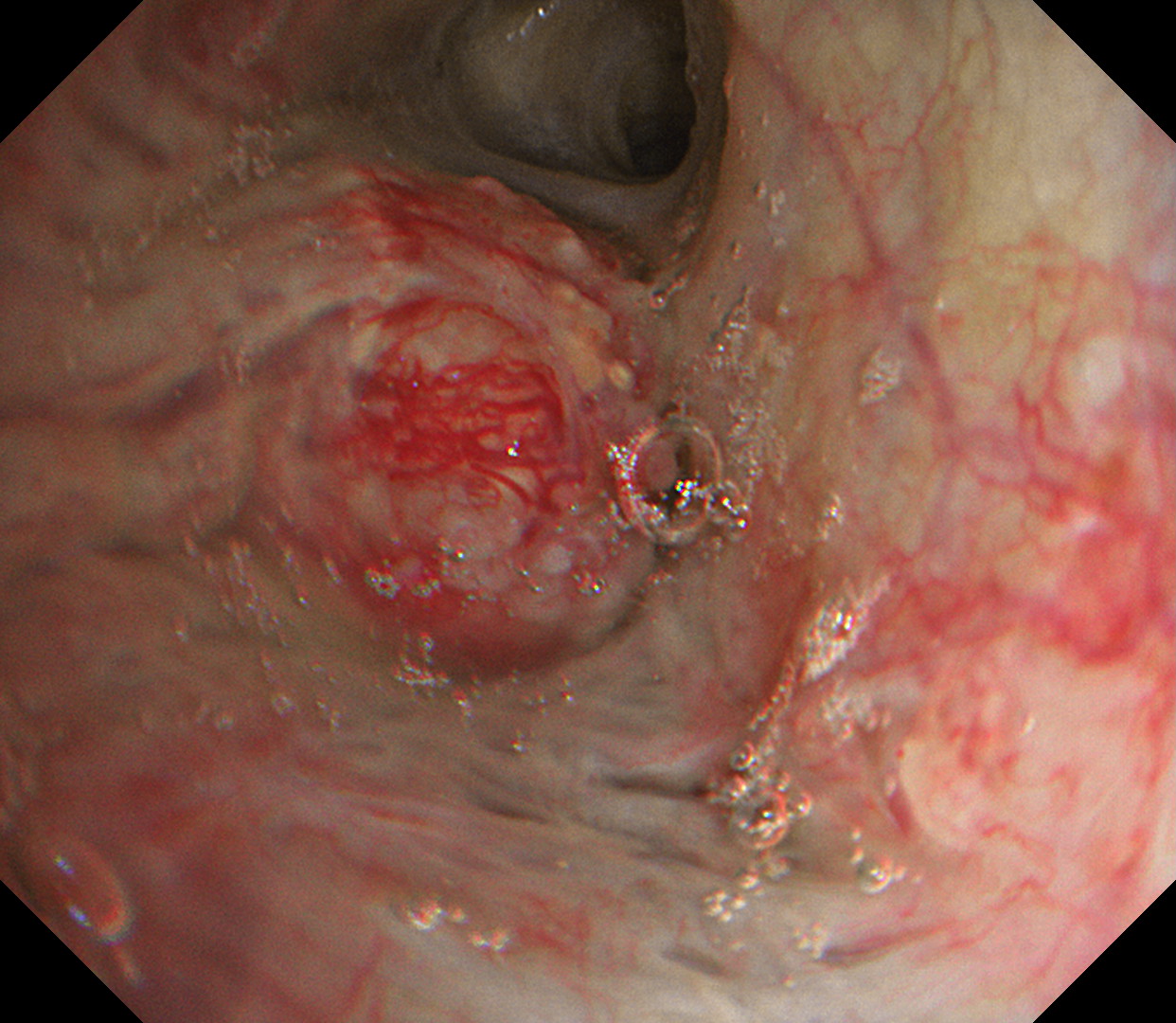
When observed with Texture and Color Enhancement Imaging (TXI™ technology), vascular properties are enhanced, revealing a network of abnormal vessels and irregularities on the surface of the tumor as well as longitudinal mural thickening of the tumor base.
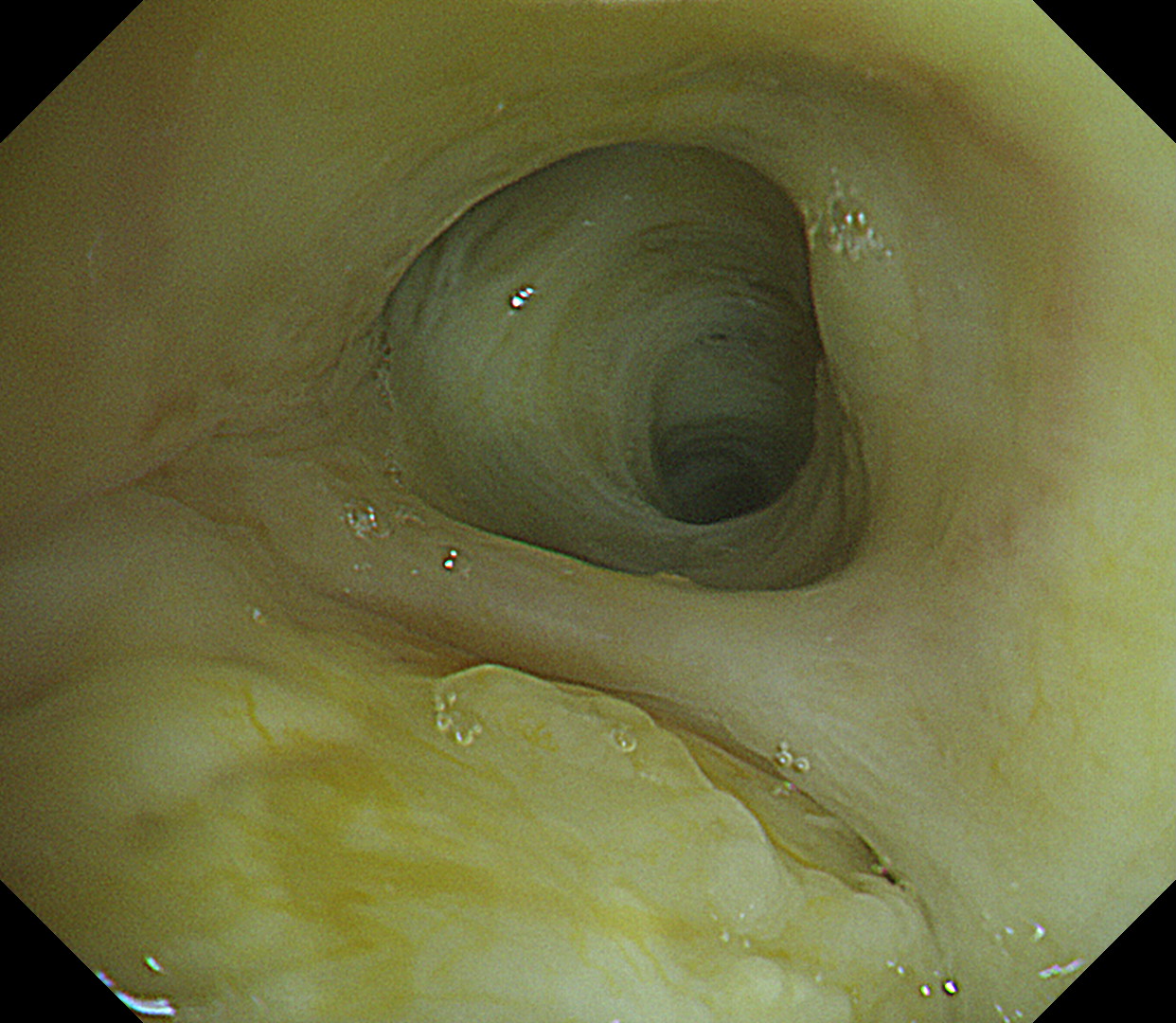
3. Close-up image of the left lower lobe lung cancer (WLI)
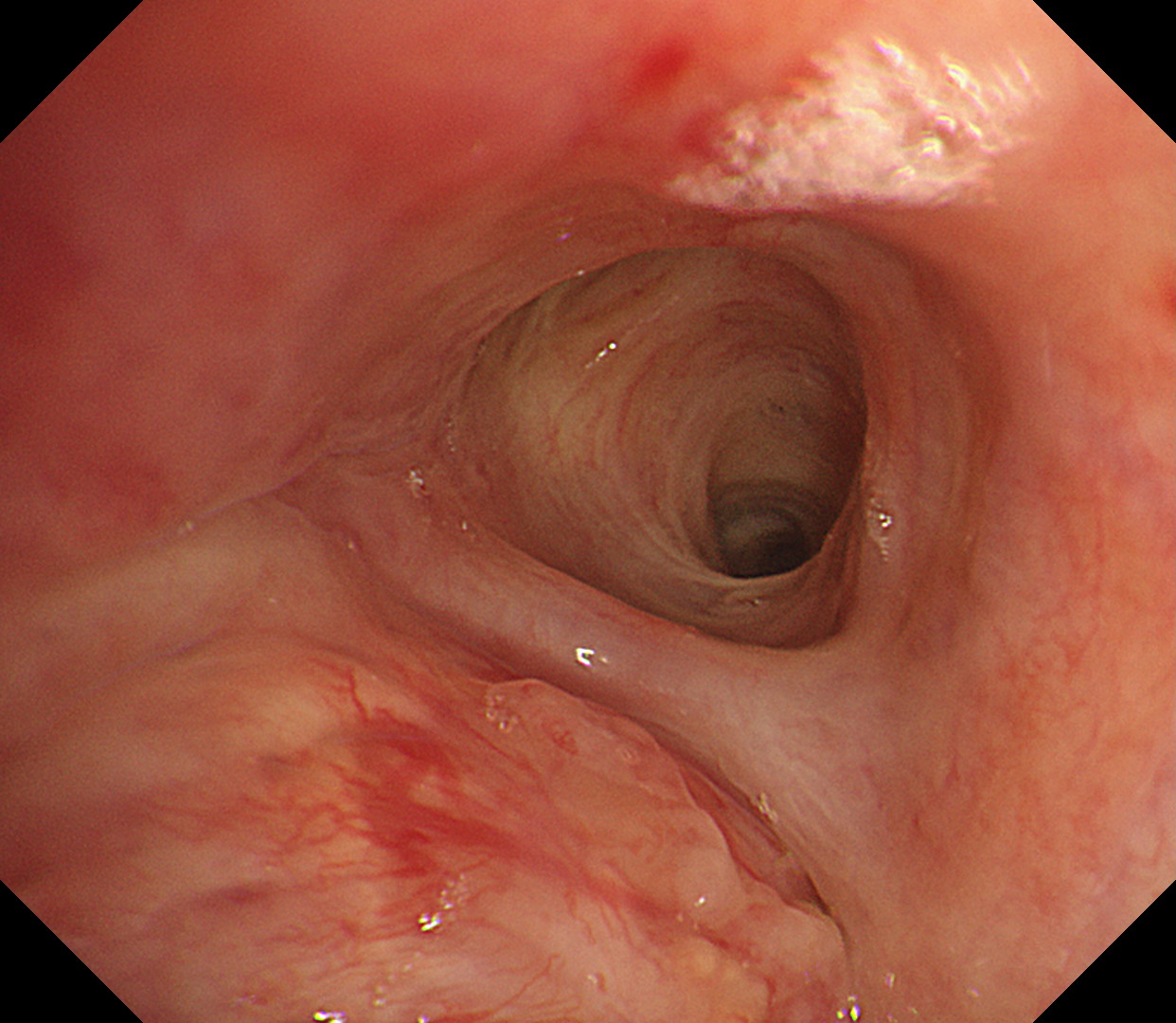
Observation with white light imaging demonstrates that the tumor is blocking the entrance of the left lower lobe but the epithelium and form of the secondary carina are maintained.
4. Close-up image of the left lower lobe lung cancer (TXI™ Technology)
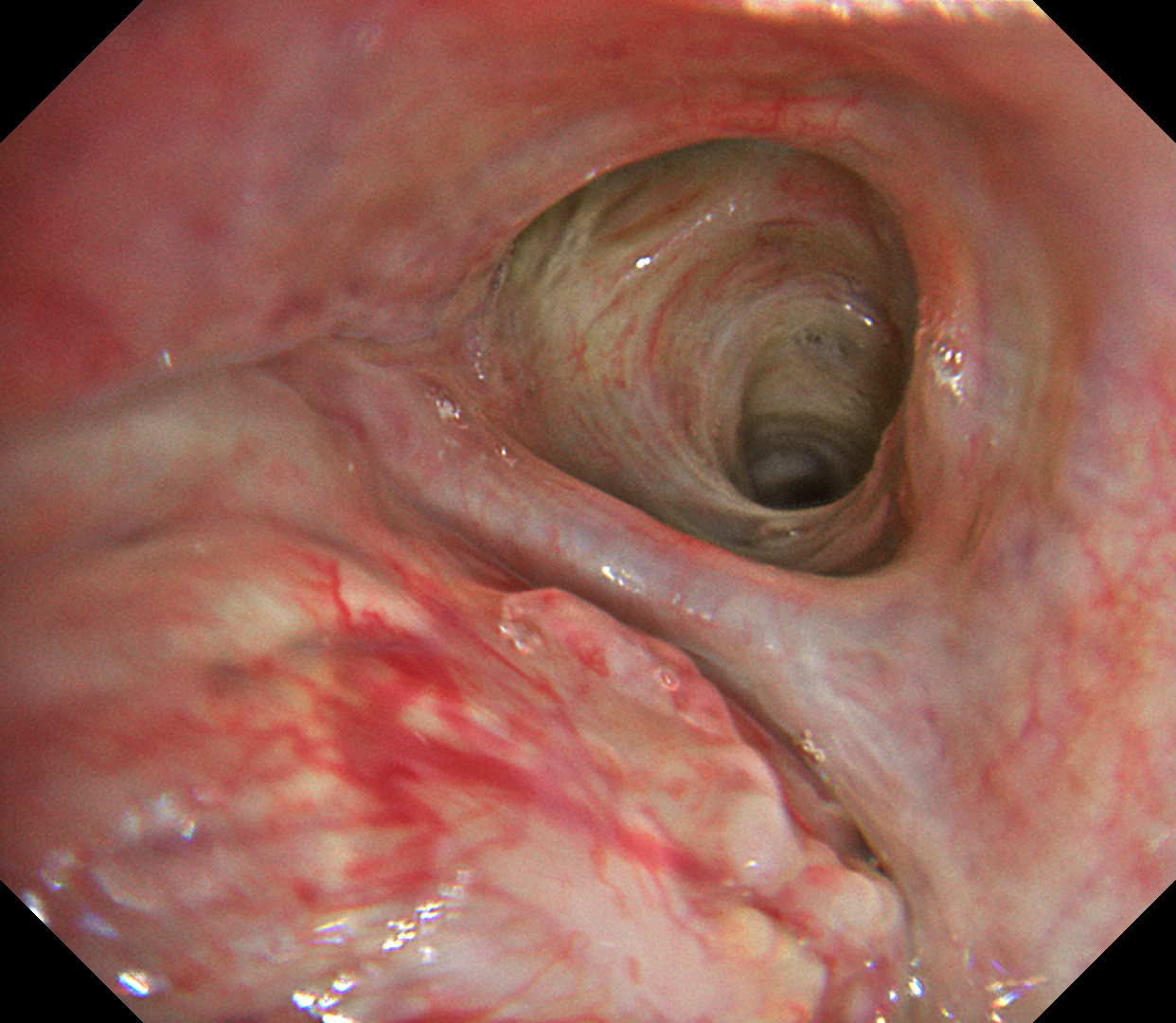
Although the tumor is blocking the entrance of the left lower lobe, the epithelium and form of the secondary carina are maintained except the part in the lower left of the image.
5. Close-up image of the left lower lobe lung cancer (RDI™ Technology)
When observed with Red Dichromatic Imaging (RDI™ technology), no active bleeding is recognized.
6. Close-up image of the left lower lobe lung cancer (NBI™ Technology)
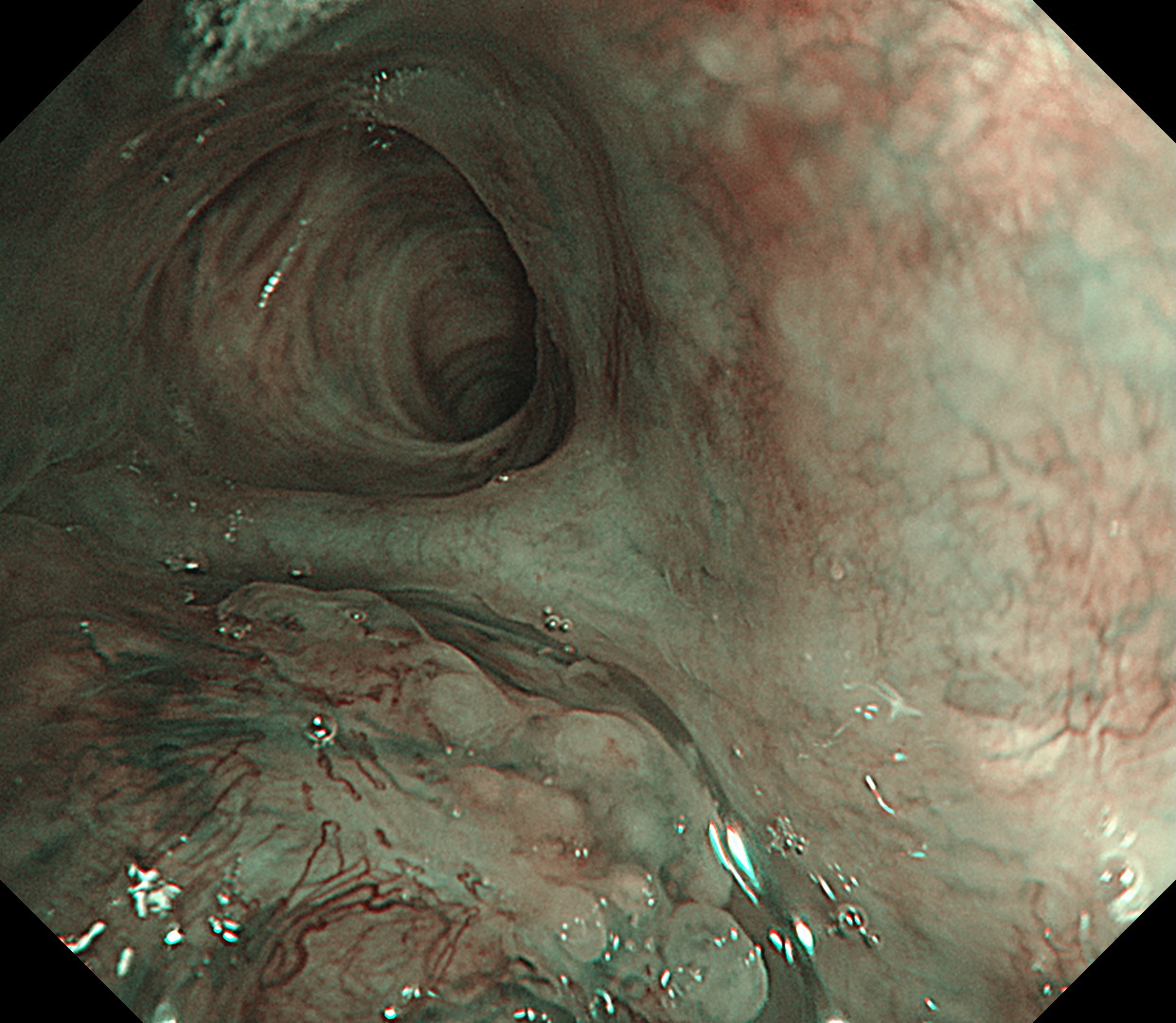
The abnormal vessels on the tumor surface and beneath it can be observed clearly with Narrow Band Imaging™ (NBI™ Technology).
Case video
In comparison with conventional white light imaging, the TXI™ technology mode noticeably enhances the properties and distribution of vessels on the surface of the tumor, as well as the characteristics of the longitudinal wall, thereby providing images that facilitate assessment of the degree of infiltration of the tumor into the bronchial wall.
Pathological Findings
Squamous cell lung cancer (resected specimen findings)
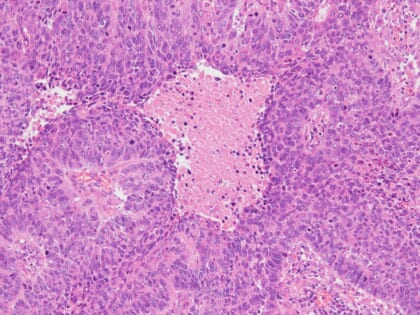
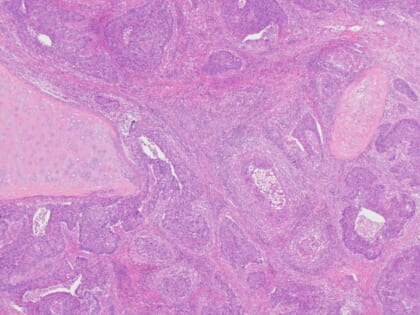
Tumor cells of various sizes are proliferating in a honeycomb or sheet-like pattern. Necrosis occurs in some cells. The tumor cells have a short spindle-shape and large polygonal cytoplasm, as well as polygonal nuclei. The tumor has infiltrated into the bronchial cartridge and lymph nodes.
Overall Comment
We performed a bronchoscopy to examine the feasibility of resection. While the image quality of white light images was extremely clear, using the TXI™ technology mode enhanced the vascular properties, highlighting the network of vessels on the tumor surface and the thickening of the longitudinal wall, thereby facilitating comprehension of the characteristics of the lesion and the extent of infiltration. It was finally determined that resection would be feasible. We subsequently performed left lower lobe sleeve resection and mediastinal lymph node dissection. The cytological examination of the resected bronchial stump was negative.
Co- author
Department of Internal Medicine, Miyazaki Prefectural Miyazaki Hospital
Dr. Gen-ichi Tanaka, Dr. Ryoichi Matsumoto, Dr. Ritsuya Shiiba
Department of Surgery, Miyazaki Prefectural Miyazaki Hospital
Dr. Kiichiro Beppu, Dr. Seiichi Odate
Department of Anatomic Pathology, Miyazaki Prefectural Miyazaki Hospital
Dr. Kousuke Marutsuka, Dr. Murasaki Aman
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer
- Content Type