Kei Morikawa, MD
Division of Respiratory and Infectious Diseases
Department of Internal Medicine
St. Marianna University School of Medicine
Disclaimer:
- TXI™, RDI™, NBI™, and BAI-MAC™ Technologies are not intended to replace histopathological sampling as a means of diagnosis
- The positions and statements made herein by Dr. Morikawa are based on Dr. Morikawa’s experiences, thoughts and opinions. As with any product, results may vary, and the techniques, instruments, and settings can vary from facility to facility. The content hereof should not be considered as a substitute for carefully reading all applicable labeling, including the Instructions for Use. Please thoroughly review the relevant user manual(s) for instructions, risks, warnings, and cautions. Techniques, instruments, and setting can vary from facility to facility. It is the clinician’s decision and responsibility in each clinical situation to decide which products, modes, medications, applications, and settings to use.
- The BF-1TH1200 used in this case is not available in the US market at this time nor is there an established time for its release. The safety and effectiveness of this product and or the use of these products has not yet been established in the United States market.
- The EVIS X1™ endoscopy system is not designed for cardiac applications. Other combinations of equipment may cause ventricular fibrillation or seriously affect the cardiac function of the patient. Improper use of endoscopes may result in patient injury, infection, bleeding, and/or perforation. Complete indications, contraindications, warnings, and cautions are available in the Instructions for Use (IFU)
- Dr Morikawa, the authoring physician(s) of this presentation, are/ is a paid consultant(s) to Olympus Corporation
Scope: BF-1TH1200
Location: Intermediate bronchial trunk
Patient information: Female in her 70s
Medical history: After removal of a thyroid tumor, coughed up blood accompanied by epigastric discomfort and saw a local doctor. No history of smoking. Chest X-ray showed a mass shadow in the right lower lobe, and she was referred to our institution for further examination.
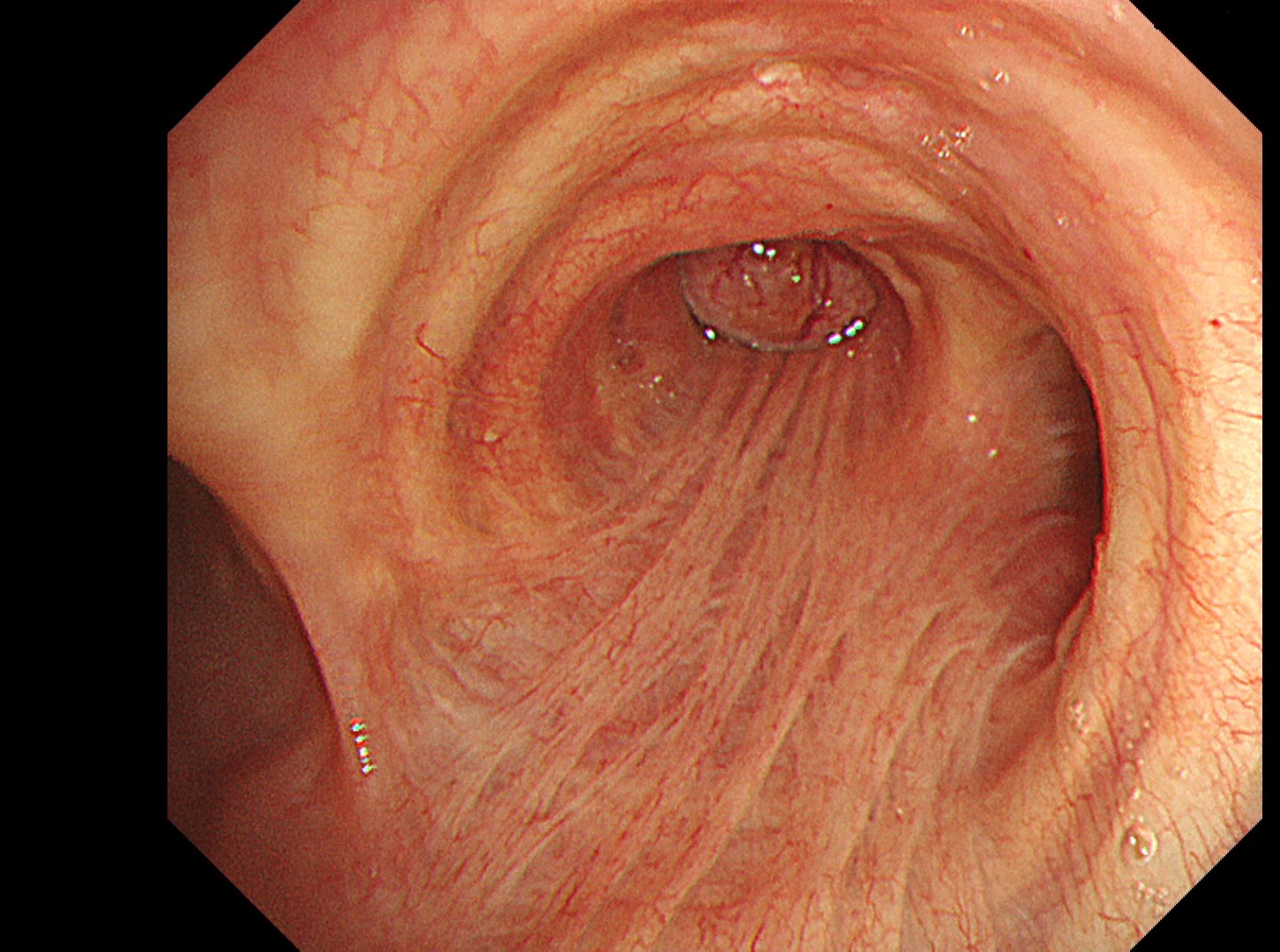
1. Right main bronchus
(WLI)
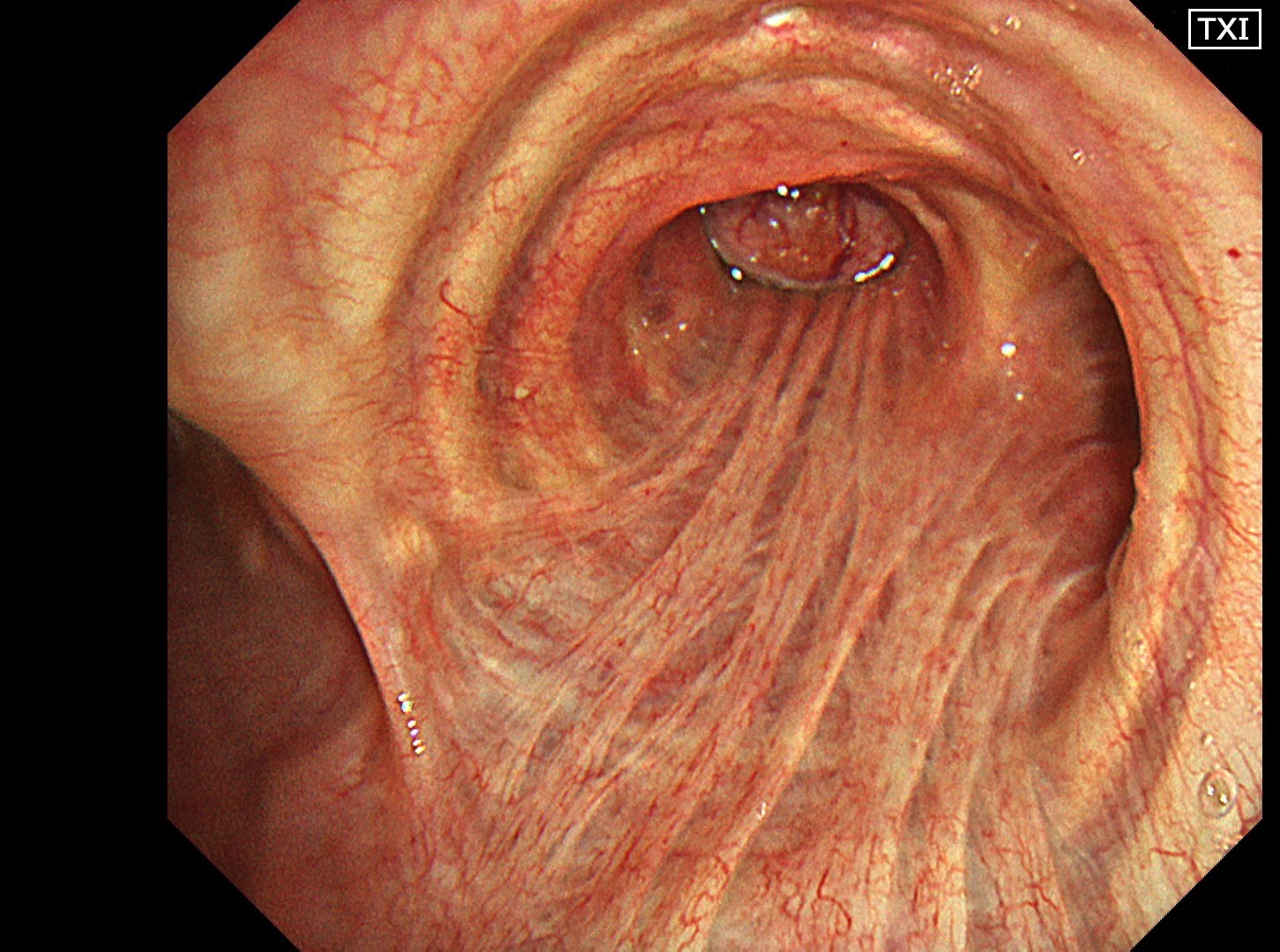
2. Right main bronchus
(TXI™ Technology - 2)
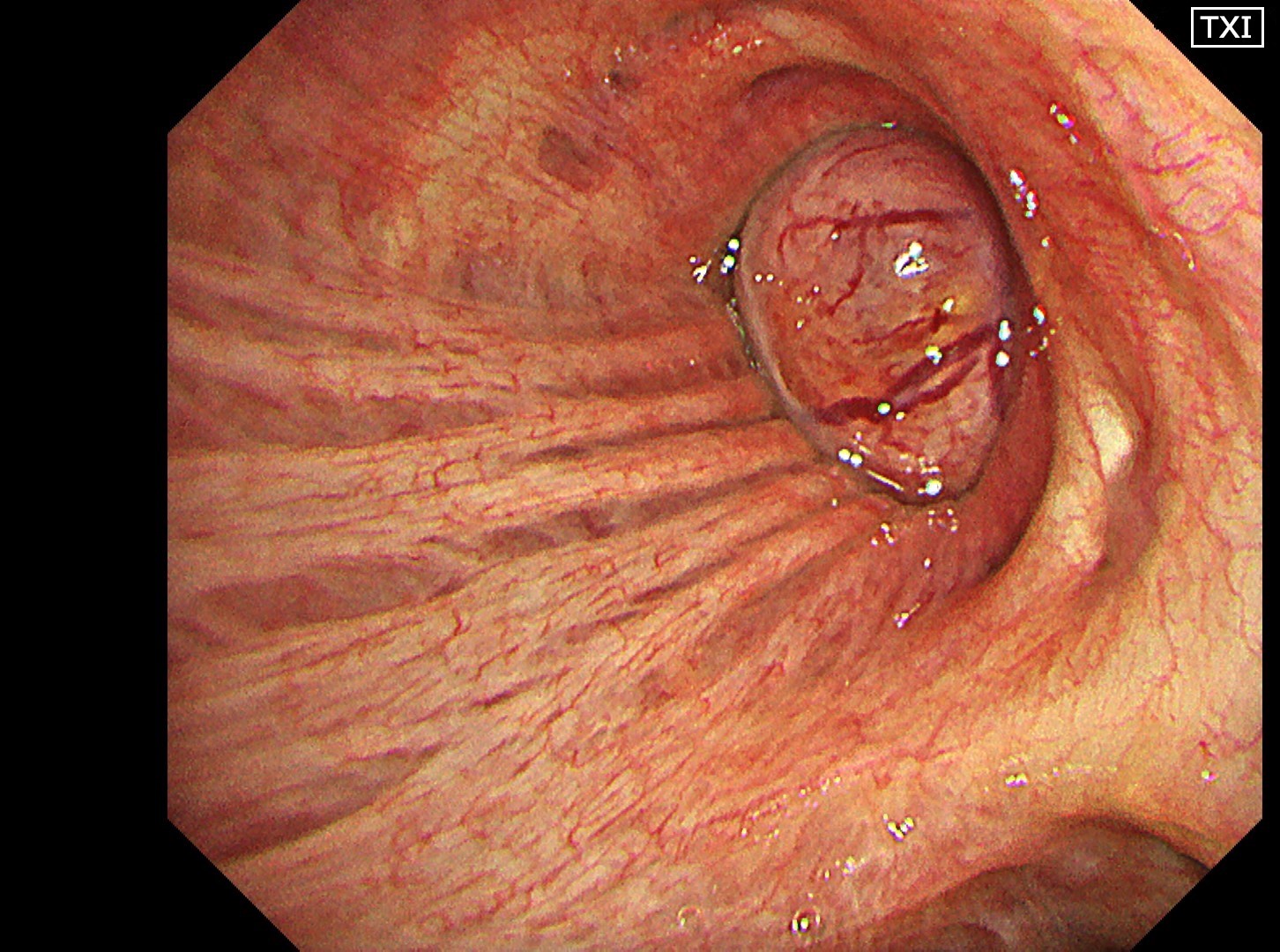
3. Intermediate trunk
(TXI™ Technology - 3)
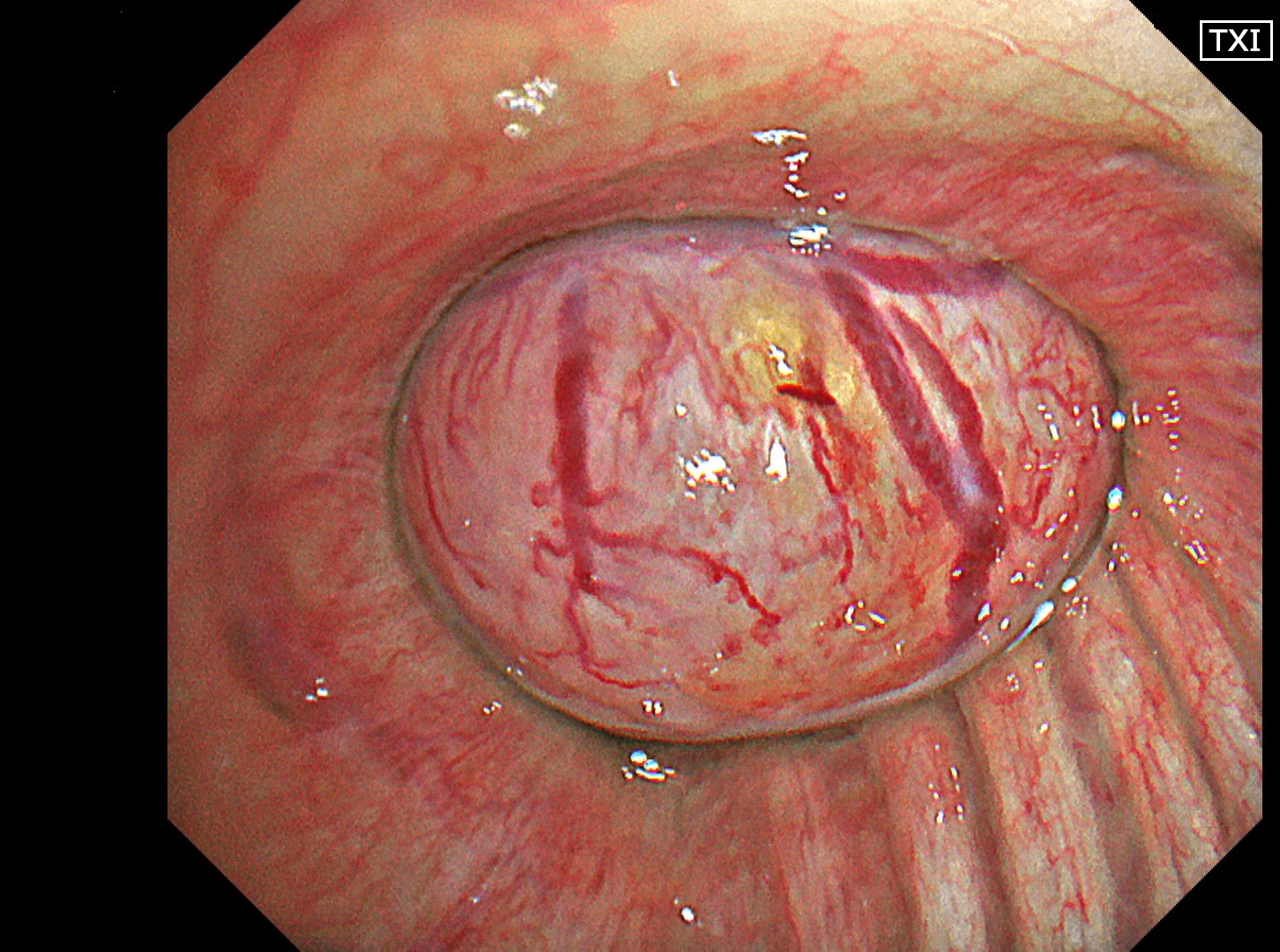
4. Intermediate trunk tumor
(TXI™ Technology - 1)
5. Intermediate trunk tumor
(NBI™ Technology)
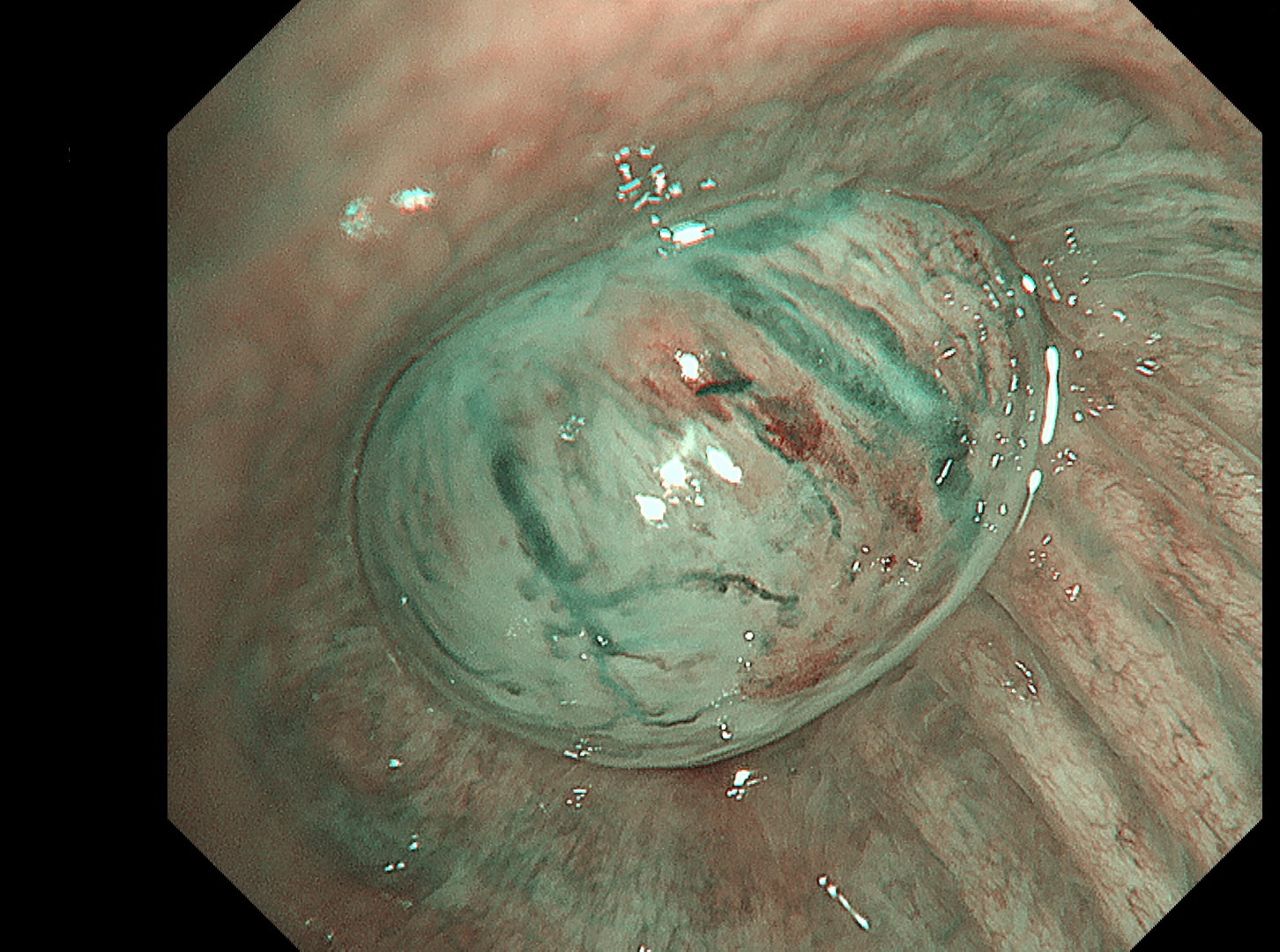
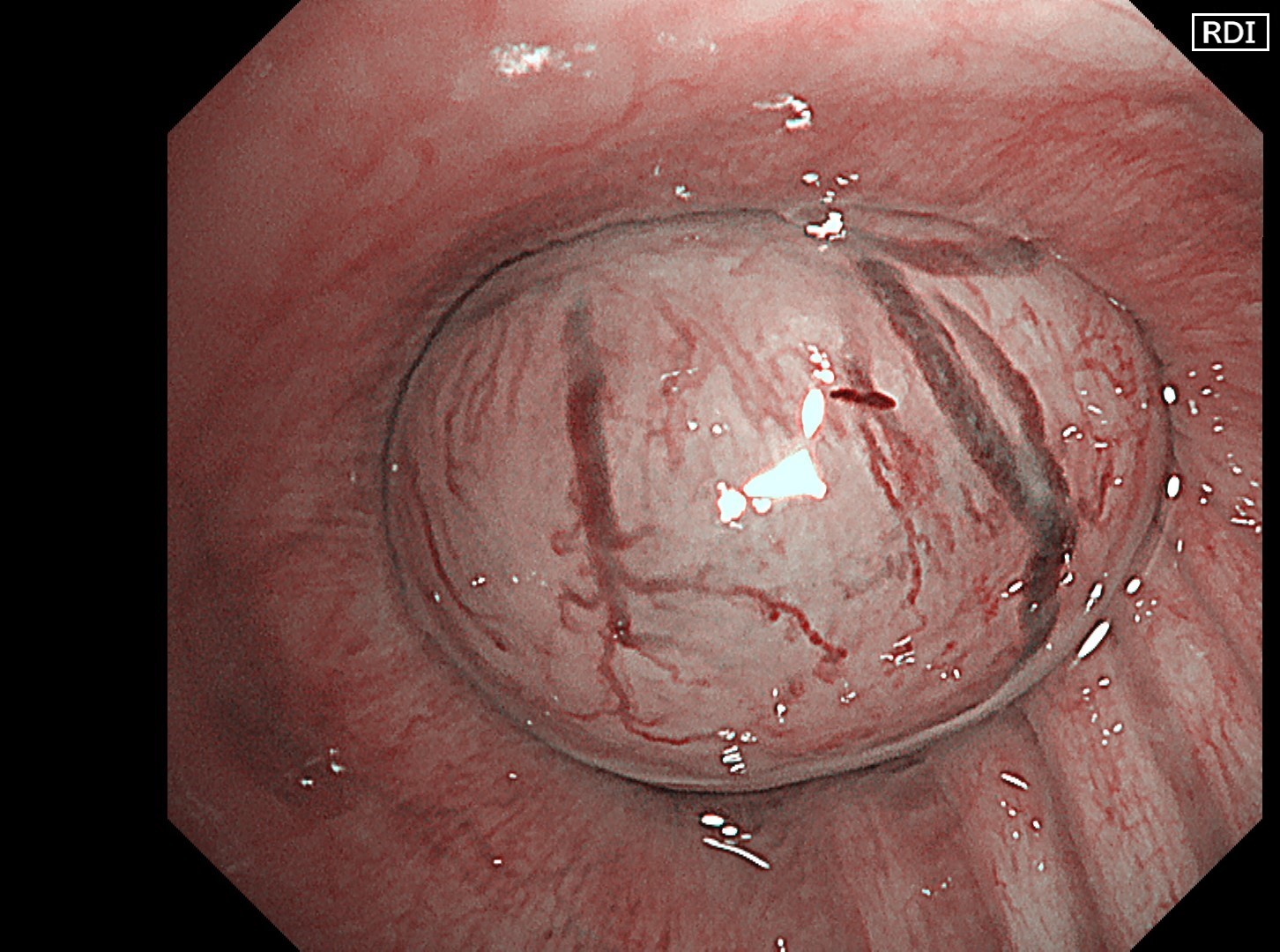
6. Intermediate trunk tumor
(RDI™ Technology - 2)
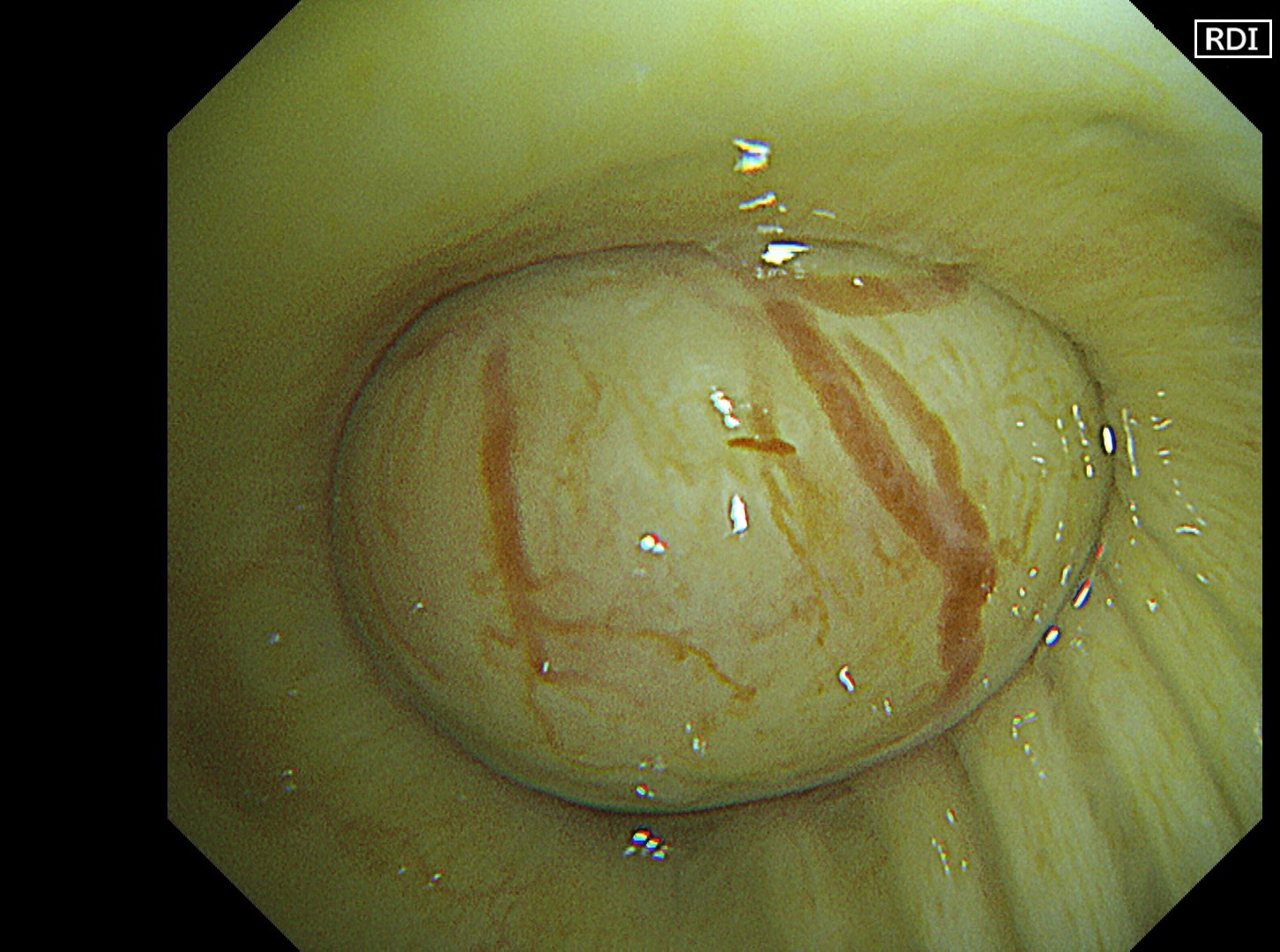
7. Intermediate trunk tumor
(RDI™ Technology - 3)
Case Video
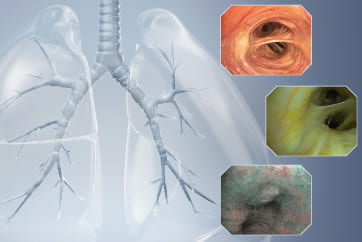
Normal structures in the vicinity of the tracheal bifurcation are observed in WLI and TXI™ technology for comparison, then the tumor in the right intermediate trunk is observed in detail in WLI™, NBI™, TXI™, and RDI™ technologies.
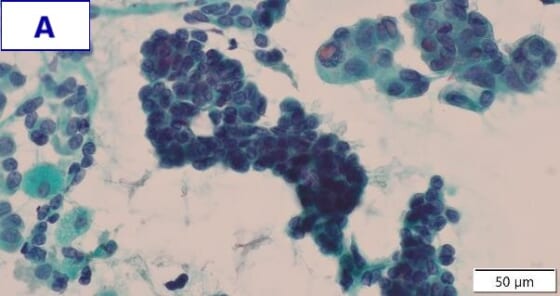
Pathological Findings
The tumor biopsy was performed using the peripheral approach to avoid bleeding.
- Figure A (Papanicolaou staining): Clusters of glandular cells with atypical morphology can be seen. These feature a high nuclear-to-cytoplasmic ratio, irregularly shaped nuclei, and increased nuclear chromatin.
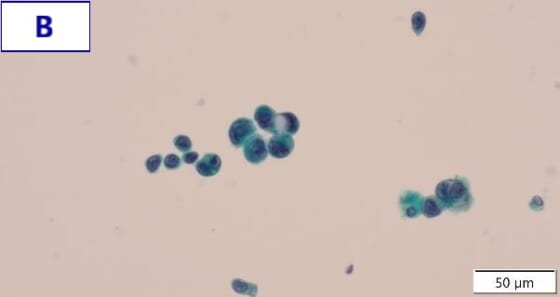
- Figure B (Papanicolaou staining): Glandular cells with atypical morphology are observed both in small clusters and scatterings. These feature unevenly distributed nuclei, a high nuclear-to-cytoplasmic ratio, and nuclear hypertrophy and irregularity.
- EGRF genetic mutation was detected by a gene mutation search.
- Final diagnosis: Primary lung adenocarcinoma (EGFR exon 21 L858R)
Overall Comment
In the comparison between WLI and TXI™ technology viewed from above the tracheal bifurcation, the peripheral lesion could be recognized first with the BAI-MAC™ technology function, which maintained the brightness of the lesion. TXI™ technology observation increased the visibility not only of the lesion but also the normal structures in the trachea and bronchi. In this respect, the value of high-specification equipment has been shown. Subepithelial vessels characteristic of tumors were most clearly depicted with the TXI™ technology and RDI™ technology settings. Since there were no significant invasion findings, low-grade malignancy was taken into consideration, and the lesion was designated as an EGFR-mutant lung adenocarcinoma. Molecular-targeted medication demonstrated high efficacy.
Co-editor:
Dr. Nobuyuki Ohike
Department of Pathology, St. Marianna University School of Medicine
- Content Type