Urology and Oncology Clinic
Lek. Jakub Kempisty
Introduction
Urolithiasis is a common condition affecting more than 10% of the population of well-developed countries.
The most common clasification of stones consists of:
• Stones unrelated to urinary tract infections
• Stones associated with urinary tract infection
• Hereditary urolithiasis
• Drug-induced stones
In addition, stones can be classified based on:
• Size of the Concrement
• Location of the Concrement
• Etiology of occurrence
• Stone Composition
• Recurrence risks
The diagnostic assessment prior to treatment of urinary tract stones should include a CT scan. Performing abdominal CT scan with contrast prior to PCNL surgery procedure facilitates access planning and shortens operative time.
Urinary tract stones in the renal pelvicalyceal system are called staghorn calculus (stones).
Depending on the collecting system’s occupancy level they can be:
• Partial – when stones occupy the renal pelvis and at least two calyxes
• Complete – when stones occupy the entire pelvicalyceal system
• Total – when stones occupy the entire pelvicalyceal system with secondary hydronephrosis
In about 50 % of cases, staghorn calculi are infection stones, commonly referred to as struvite stones.
Struvite stones are composed of magnesium, ammonium and phosphate compounds.

Fig.1. Instruments / Equipment

Fig.2. Creating surgical access

Fig.3. Creating surgical access

Fig.4. Puncture of the pelvicalyceal system
Other risk factors associated with staghorn calculus formations include urinary obstruction, anatomical variations, longterm urinary catheterisation and urinary diversion procedures performed in the past.
Nowadays, when dealing with staghorn calculus or large kidney stones PCNL procedure is the treatment of choice. The procedure uses flexible or rigid endoscopes. Smaller sized nephroscopes of 22 Fr and less, so-called mini-PCNL are becoming increasingly popular.
The main contraindications for PCNL treatment include:
• Untreated urinary tract infection
• Tumour in the presumptive access tract area
• Potential malignant kidney tumors
• Pregnancy
• Uncontrolled bleeding disorders
It is important to rule out and possibly treat a urinary tract infection before treatment of kidney stones.
The PCNL technique is a relatively safe procedure. The main complications following PCNL include fever, haemorrhage, complications related to chest trauma, sepsis.
Approximately 100 procedures per year using PCNL technique are performed at the Urology Clinic at the University Clinical Hopsital No. 1 in Rzeszów. In the vast majority of cases it is necessary to perform intracorporal lithotripsy during the procedure. For stone fragmentation we usually use the ShockPulse sonotrode from Olympus Company. By producing ultrasonic waves and ballistic shock waves this sonotrode offers dual action lithotripsy for achieving the optimal effect. The device is additionally equipped with an integrated suction channel for removal of stone dust. The use of state-ofthe- art solutions contributes to a significant reductions in operative time compared to typical mechanical lithotriptors. Shortening the length of surgery has a significant impact on improving the safety profile with reduced perioperative and post-operative complications. Recently, we also had the opportunity to perform procedures using miniaturised Mini- PCNL equipment from Olympus Company. According to the guidelines of European Association of Urology, the use of mini-PCNL of sizes smaller than 22 Fr lowers the risk of perioperative complications, without jeopardizing the effectiveness of the performed procedures.
There were no complications reported after procedures performed on our patients with the use of Mini – PCNL equipment. The use of tubeless technology during surgery contributed to shorter length of hospital stay and patients’ faster recovery.
With appropriate patient selection, procedures carried out with the Mini-PCNL should be standard approach performance canon.
With the Olympus Schock-Pulse, we can perform effective lithotripsy in a timely manner even when dealing with complete staghorn calculi. The images from our case report of 30-year-old patient with complete renal staghorn calculi, which was treated with lithotripsy are presented below. A stone was composed mainly of calcium phosphate with a density of 2000 Hounsfield units. Thanks to the use of a sonotrode, there were no complications after the procedure, while the patient was discharged from the Urology Clinic on postoperative day 3 with achieved complete stone removal.
CT images of urolithiasis
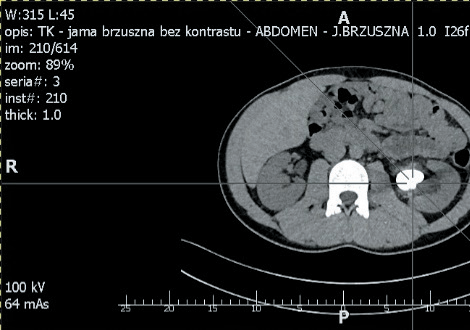
Fig.1A.

Fig.2A.
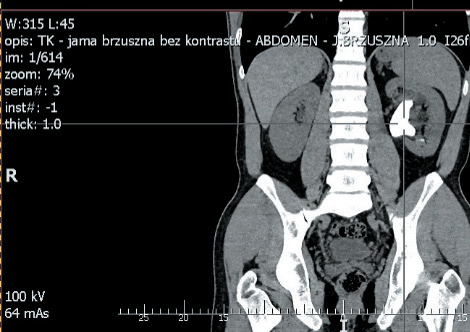
Fig.3A.
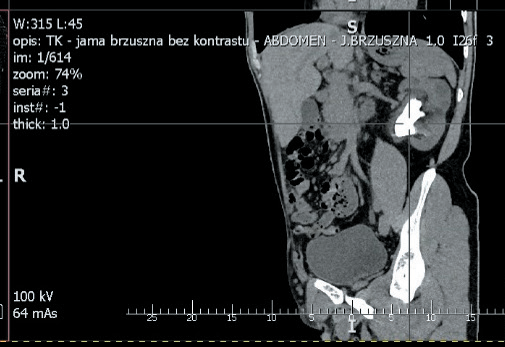
Fig.4A.
Conclusions
In summary, modern technologies are an evolving part of urological management. The use of new medical solutions help us to minimise the risk of serious complications and provides us with the possibility of minimally invasive treatment of cases for which, until now, conventional open surgery might have been the only option. Thanks to these solutions our patients may be offered options that closely match their expectations in terms of shorter recovery times and fewer serious complications.
- Content Type