Disclaimer
This surgical technique is presented to demonstrate the technique utilized by:
A. Simon Carney
Professor of Otolaryngology – Head & Neck Surgery, Flinders University, Adelaide, Australia.
Brent A. Senior
Nathaniel and Sheila Harris Distinguished Professor of Otolaryngology, University of North Carolina at Chapel Hill, USA.
Olympus as manufacturer does not practice medicine, and therefore the information on the products and procedures contained in this document is of a general nature and does not represent and does not constitute medical advice or recommendations. This information does not purport to constitute any diagnostic or therapeutic statement with regard to any individual medical case. Each patient must be examined and advised individually, and this document does not replace the need for such examination and/or advice in whole or in part.
Please refer to the instructions for use for important product information, including, but not limited to, contraindications, warnings, precautions, and adverse effects.
Procedure Steps
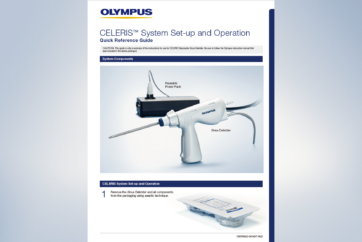
01 Set Up
The following is intended as a basic equipment list. Most surgeons will use several more instruments routinely. Even the most basic endoscopic sinus surgery will be difficult, if not impossible without these instruments being present on the surgeon’s tray:
Freer elevator
Small back biting forceps (fixed or rotating)
Straight Blakesley-Weil forceps
45º Blakesley-Weil forceps
Straight sinus thru-cut forceps
45º sinus thru-cut forceps
Double right angle ball probe
2mm forward slanting Kerrison punch forceps
Straight curette
Angled frontal curette
45º curette
Olive – tip angled suction
Disposable straight suction
Diathermy instrument: suction bipolar ideal but long–tine bipolar forceps will suffice
Microdebrider

Due to the risk of neck and back injury, the vast majority of surgeons now operate off the screen or video monitor. The patient’s head should be placed on a soft head ring and, if under general anaesthetic, the conjunctivae should be lubricated and can be taped laterally or left open, as per the surgeon’s individual preference. The operative table should be reversed to allow space for the surgeon’s legs to sit under the table. Depending on the size of the patient, an arm board may be helpful, placed alongside the head of the bed and covered with two or more rolled up sheets to elevate the surgeon’s elbow 2-3 inches above the height of the bed.
Anti-Fog:
A simple detergent solution may suffice although if a commercially–available anti-fog agent is used, this can either be on a sponge placed on the patients forehead or beside the surgeon. Another option is to place the anti-fog agent into a 2ml syringe with the plunger removed and the black rubber plunger seal then reinserted into the barrel of the syringe. The syringe barrel is of an ideal size to place an endoscope. This minimises the risk of blood contaminating the anti-fog sponge and also minimises excessive hand movements.
Orientation:
There should be a direct line between the surgeon’s eyes, the nostrils of the patient and the centre of the video monitor. This will prevent excessive neck or back rotation and minimise the risk of strain, especially important for prolonged procedures.
Preparation:
Anti-coagulation medication should be stopped at an appropriate time prior to surgery. Homeopathic or over the counter medication such as fish oil, glucosamine and multi vitamins should also be stopped 7-10 days prior to surgery. If the procedure is to be performed under local anaesthetic or LA and sedation, the nose should be first anaesthetised with lignocaine/lidocaine, with or without phenylephrine. Under general anaesthetic it is usually not required and local anaesthetic/decongestant swabs or pledgelets can be placed without spray. Depending on the planned surgery, either 4 or 6 neuropatties/strips of 5x1cm ribbon gauze are used.
Where available:
10% Cocaine solution (max dose is 3mg/kg), 1ml 1:1000 adrenalin, 6ml normal saline.
Where cocaine is not available:
The ribbon gauze or neuropatties are soaked thoroughly in the solution. Using the 0° endoscope, one gauze is placed in the middle meatus, covering the uncinate process and extending over the axilla of the middle turbinate. Another is placed between the middle turbinate and the septum and a third (if required) is draped over the inferior turbinate. Once the gauze has been removed, further topical vasoconstriction can be achieved using 2% lignocaine/lidocaine with adrenalin. The middle turbinate itself and the frontal process of the maxilla are optimal injection sites. Enough anaesthetic should be applied to ensure blanching of the required area with a maximum of 2ml used on each side of the nose.

- Keyword
- Content Type