05 The Frontal Recess
Ensure a complete uncinectomy has been performed.
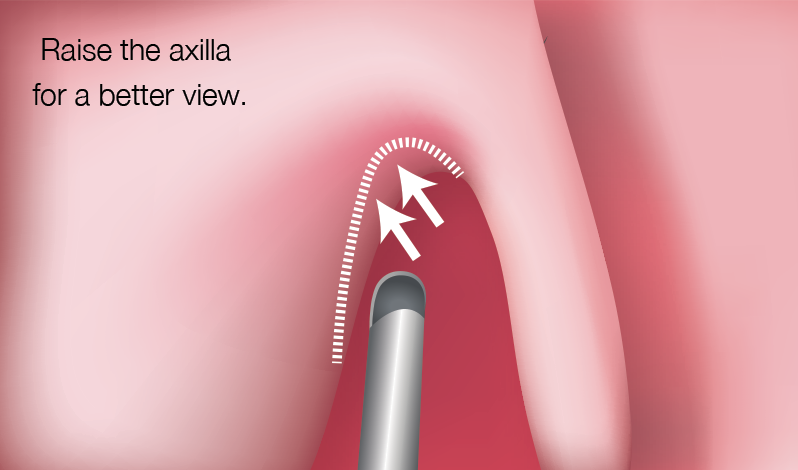
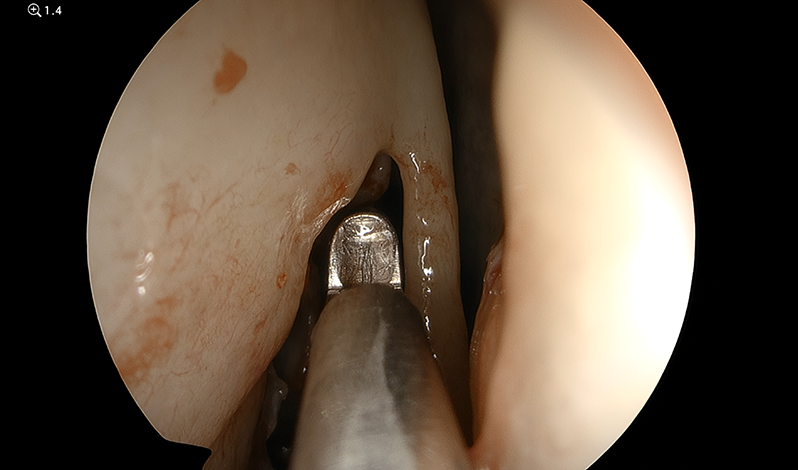
To improve access to the frontal recess, enlarge the axilla of the middle turbinate using a 2mm Kerrison punch. This will remove the anterior face of the agger nasi cell and also the hard bone of the frontal process of the maxilla.
Notes:
It is important to ensure the Kerrison punch does not expose the lateral sac at this point. By balloting the eye, the surgeon can be reassured that the lamina papyracea is intact and then a microdebrider can be used to remove the fragments of the axilla.
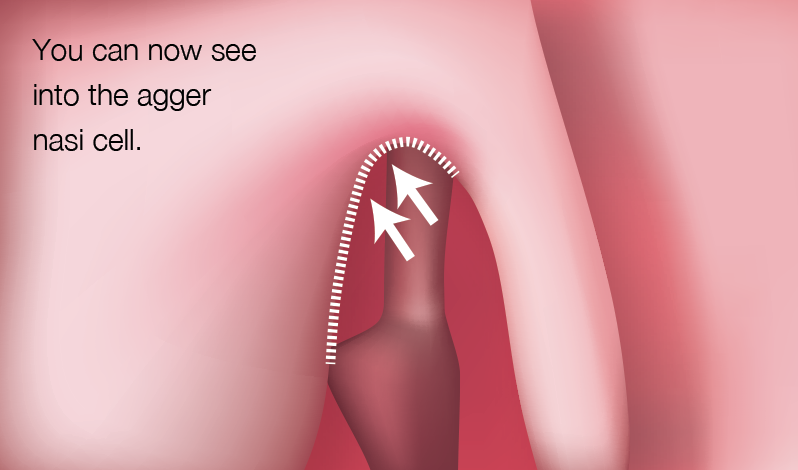
The surgeon should then be looking directly into the agger nasi cell and visualising its posterior wall. The preoperative CT scans can be examined to identify the frontal drainage pathway. This is always posterior to the agger nasi cell but may be further complicated by the presence of fronto-ethmoidal cells (Kuhn cells). Use of a frontal sinus seeker at this point may clearly identify the frontal drainage pathway.
Notes:
Not all patients have an agger nasi cell. It is important to review the preoperative CT scan to identify this cell.
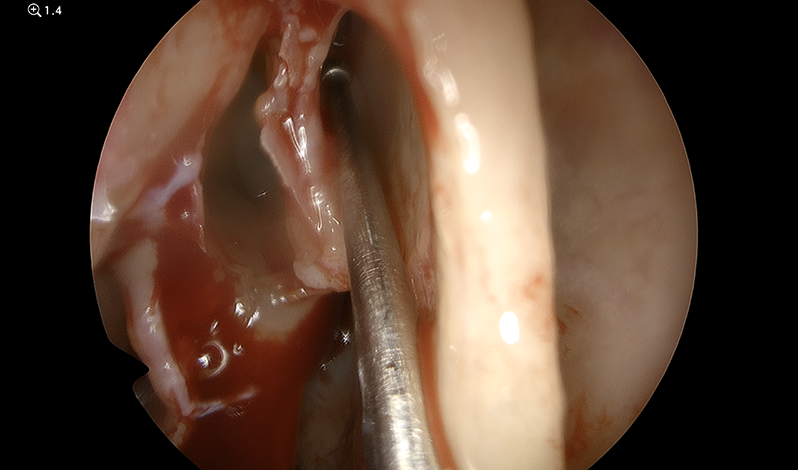
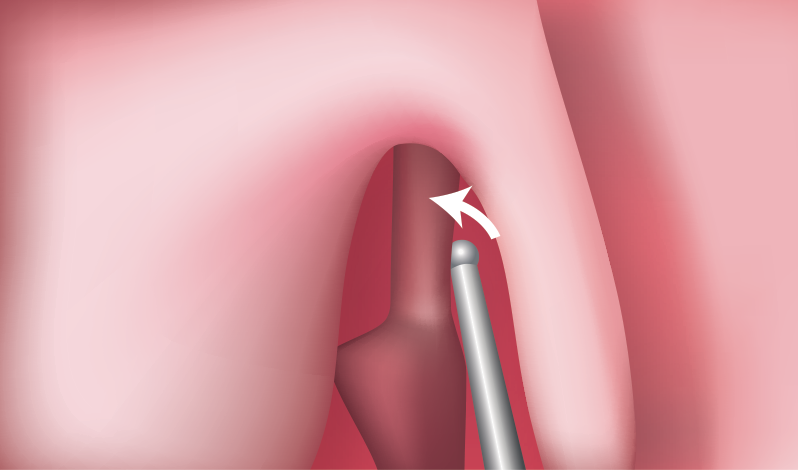
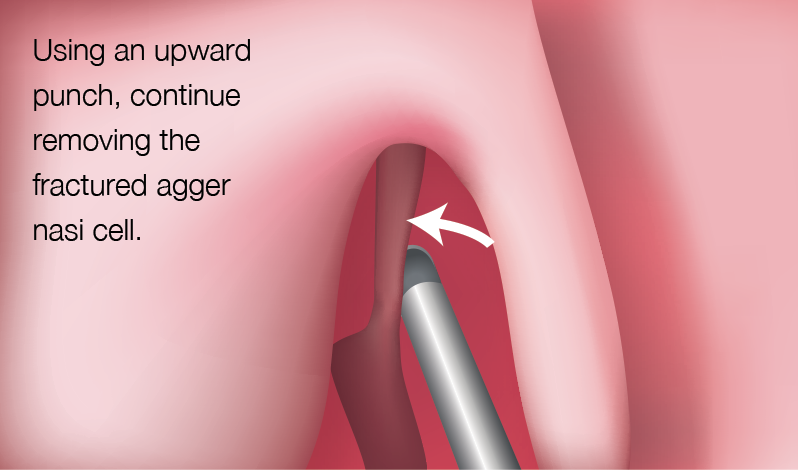
Straight and angled curettes can be used to fracture forward the posterior wall of the agger nasi cell.

Formal identification of the anterior ethmoidal artery is recommended to ensure that the skull base is not at risk.
It may be helpful for the surgeon to switch to a 30º or 45º endoscope. Angled microdebrider blades (40º, 60º or 90º degree) will also facilitate removal of the anterior frontoethmoidal cells.

Notes:
・Whilst performing the frontal recess dissection, it is critically important not to cause a circumferential mucosal injury. If this occurs, the frontal recess will stenose and may produce iatrogenic frontal disease that can be extremely difficult to salvage.
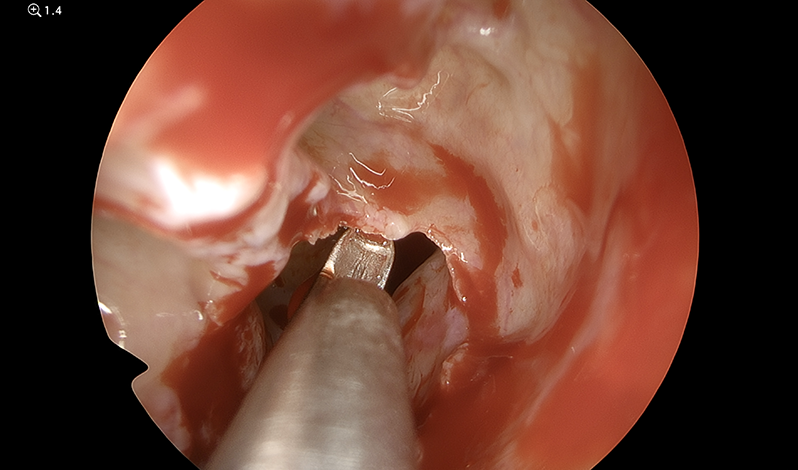
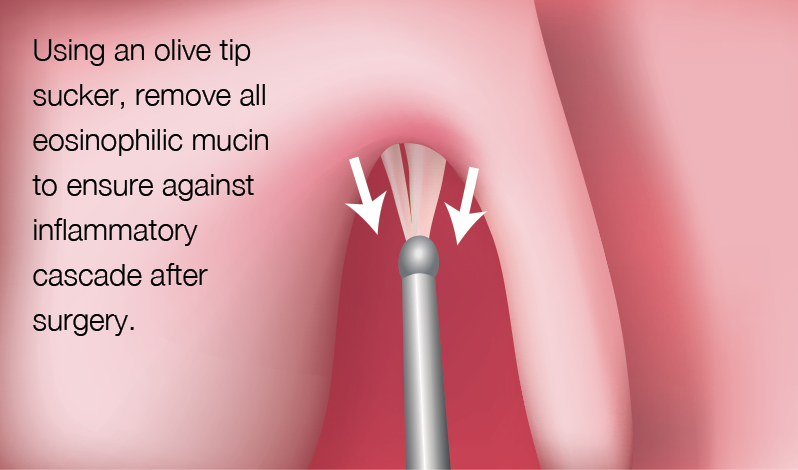
・A particularly useful instrument in the frontal recess is the 2.5mm Hosemann 70º frontal punch. This sharp punch is extremely effective in removing frontoethmoidal cells and ensuring the frontal recess is enlarged anteriorly, laterally and medially. If there are posterior cells within the frontal recess, it is important that the bone is dissected out in a blunt manner and then removed with Blakesley Weil forceps, ensuring mucosal integrity is preserved. Following an adequate frontal recess dissection, it should be possible to insert an olive tip sucker into the frontal sinus and this can be used to irrigate the sinus, remove secretions and/or debris.
- Content Type