Dr. med. Marek Czyż
General Surgery and Oncological Surgery Specialist
Head of the Operating Unit & Endoscopic Department Beskid Oncology Centre Bielsko Biała, Poland
Specialized Hospital Podkarpacki Ośrodek Onkologiczny Brzozów, Poland
Introduction
After 20 years of ERCP treatments with various plastic and metallic stents for bile ducts, I finally obtained a golden, universal tool in the form of a self-expandable metallic stent, coated silicone with holes, which – in my opinion – is suitable for both benign and malignant lesions, and can also effectively drain bile until the planned surgery. The stent in question is Hanarostent, model BMCL.
Need for Multi-Hole Stent
When Olympus announced in 2017 that a new type of stent would be added to the product portfolio, I had a 55-year-old patient with long-term chronic pancreatitis and stricture of the distal intrapancreatic biliary duct after repeated stenting with plastic stents. The patient was unfit for surgical treatment due to the general condition, and at the same time the plastic stents had become ineffective due to the residual bile sludge. The placement of an uncoated self-expandable stent was out of the question because it is irremovable. A coated stent, on the other hand, could close the gallbladder duct and cause a subsequent gallbladder inflammation after expansion.
First Experience with Multi-Hole Stent
Then, in autumn 2017, courtesy of a regional Olympus representative, as the first in Poland, I used the BMCL stent, which effectively drained thick bile and bile sludge and did not close the gallbladder duct in the same time. After staying for six months in this patient, the stent was removed without problems with the use of a polypectomy snare. The distal part of the biliary duct was dilated to such an extent that it provided effective independent bile drainage. After such a successful experience, I introduced those stents to four medical centers, where I now perform a total of around 1,200 procedures annually.
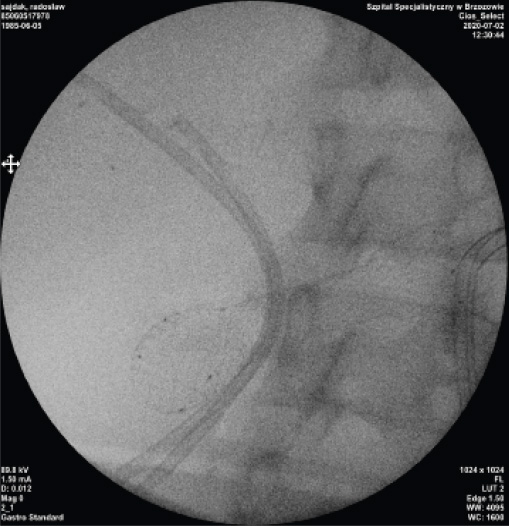
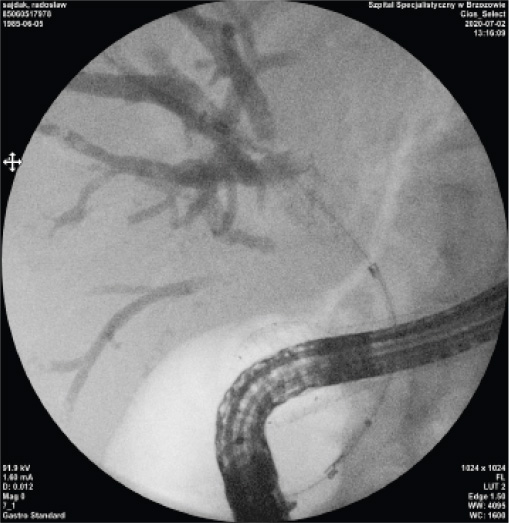
Case Presentation 1
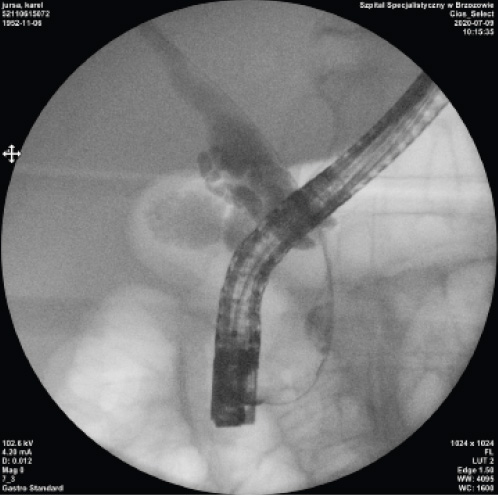
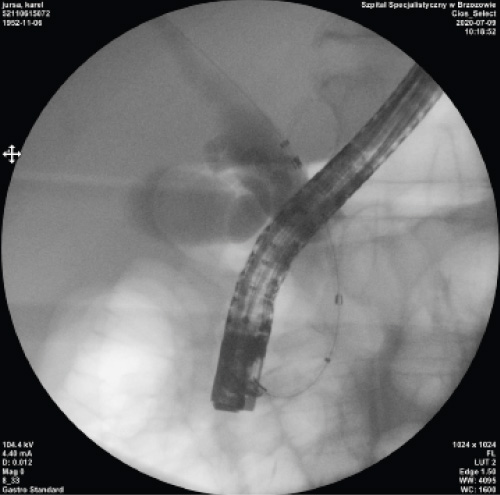
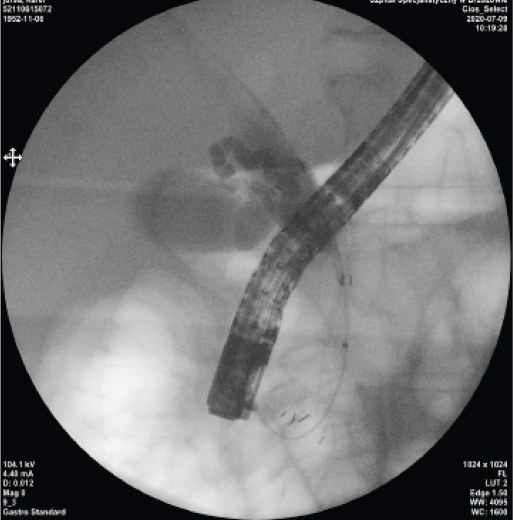
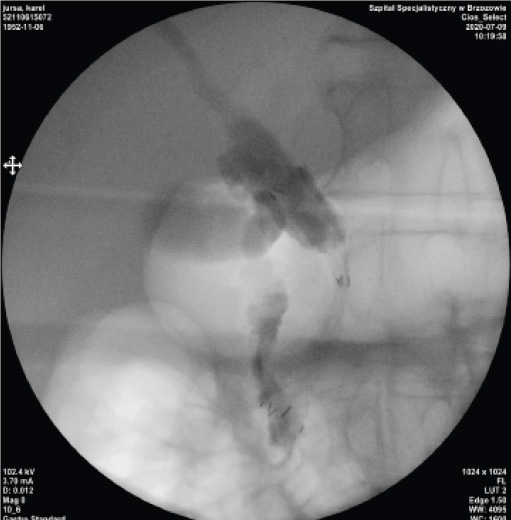
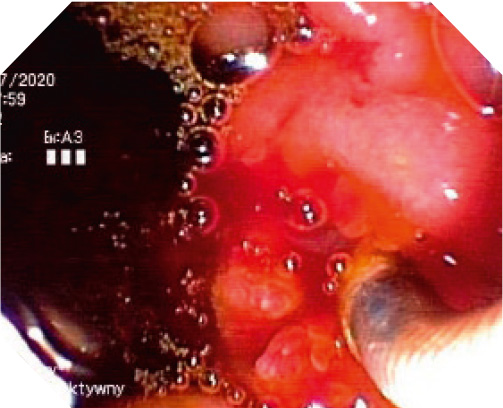
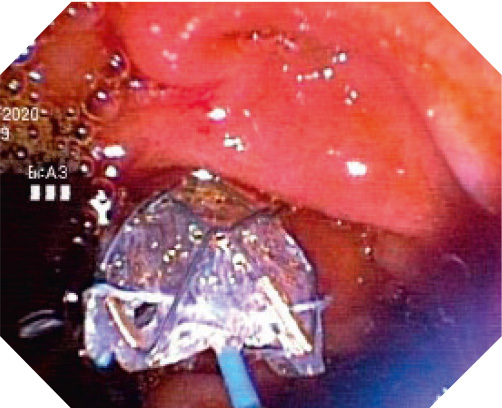
To confirm my conclusions, I present a case of a patient, 68 years old, with a surgical pancreatic head tumor and gallbladder, in whom I implanted a BMCL stent:
Case Presentation 2
I also suggest the use of BMCL stents in patients in whom it would be very difficult to reach the Vater’s papilla area, due to the high dynamics of the neoplastic process. For example, a 35-year-old patient with inoperable biliary tract tumor and a clogged duodenum due to NPL infiltration, with plastic stents used previously, theoretically without any possibility of replacing them with new ones.


In the first stage, a duodenum stent was placed. A week after the duodenal stent was placed, the descending part and the papilla region were reached through the duodenal stent and a BMCL stent was placed into the biliary tract. The cross-over biliary and duodenal stents enable the correct drainage of the bile and the movement of food content into the digestive tract.
Conclusion
The number of BMCL stents used is growing each year due to their versatility. So far I have used about 50 such stents. In benign cases, especially in chronic pancreatitis, the stent – after implantation – works as an expander that gradually widens the stricture, ensuring effective drainage of bile from the liver and gallbladder. I remove the stent after six months, obtaining dilatation of the stenosis. In neoplastic changes, when the gallbladder is removed, I use fully covered stents. In cases where the gallbladder exists, BMCL – a coated stent with holes – can be used freely. Thanks to the appearance of that stent, in my practice, uncoated stents in neoplastic lesions are gradually being replaced, as they quickly overgrow the tumor (after about three or four months) and do not provide effective bile drainage. I have not observed a BMCL stent overgrown by a tumor in my practice. It seems that the stent lumen is effectively protected by the silicone membrane.
Recently I have been using BMCL stents as a bridge in patients with existing gallbladder and jaundice and at the same time who are suitable for surgical treatment for up to several months, for example after induction chemotherapy. Effective, wide drainage without the threat of cystic duct occlusion predisposes these stents to be used in such cases.
To sum up, covered metallic stents with holes (BMCL) are very versatile in the drainage of the biliary tract in benign and neoplastic lesions, replacing other stents from the market.
As medical knowledge is constantly growing, technical modifications or changes of the product design, product specifications, accessories and service offerings may be required.
- Keyword
- Content Type