Achieving the distant view
Please read instructions for ENDOEYE FLEX DEFLECTABLE VIDEOSCOPE before use.
i Linear motion and rotational motion
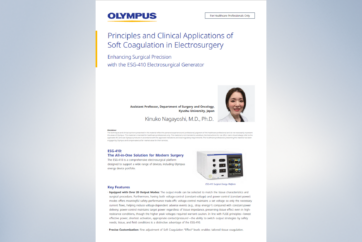
Laparoscope operation is limited by the trocar. In shifting the field of view, movement is allowed in two directions, the linear movement (backward/forward movement) along the laparoscope axis and the rotational movement (circular movement) around the fixed portion that serves as a fulcrum. According to this, the observing point is shifted. The rotational movement, in particular, is associated with the fulcrum effect: Lowering the proximal end will raise the observing point.
Figure 8 Linear motion (backward/forward motion)

Figure 9 Rotational motion (Circular movement)
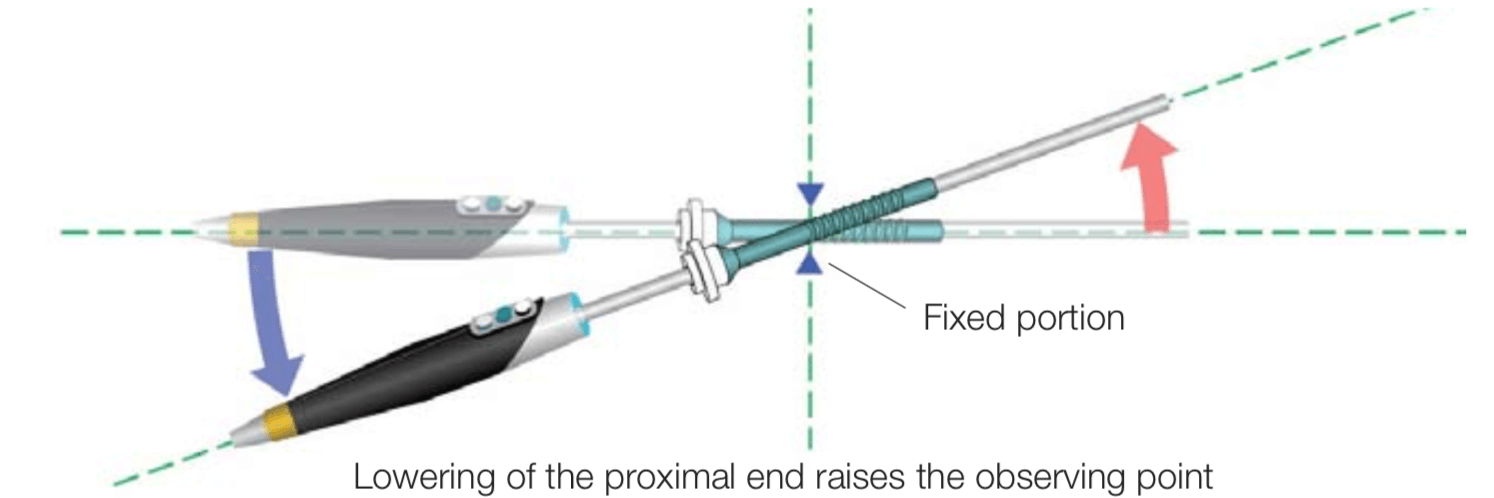
ii Distant view with forward view rigid laparoscope
With the forward view rigid laparoscope, a distant view is obtained by simple linear movement (distant view = pulling back the laparoscope).
Figure 10 Distant view with forward view
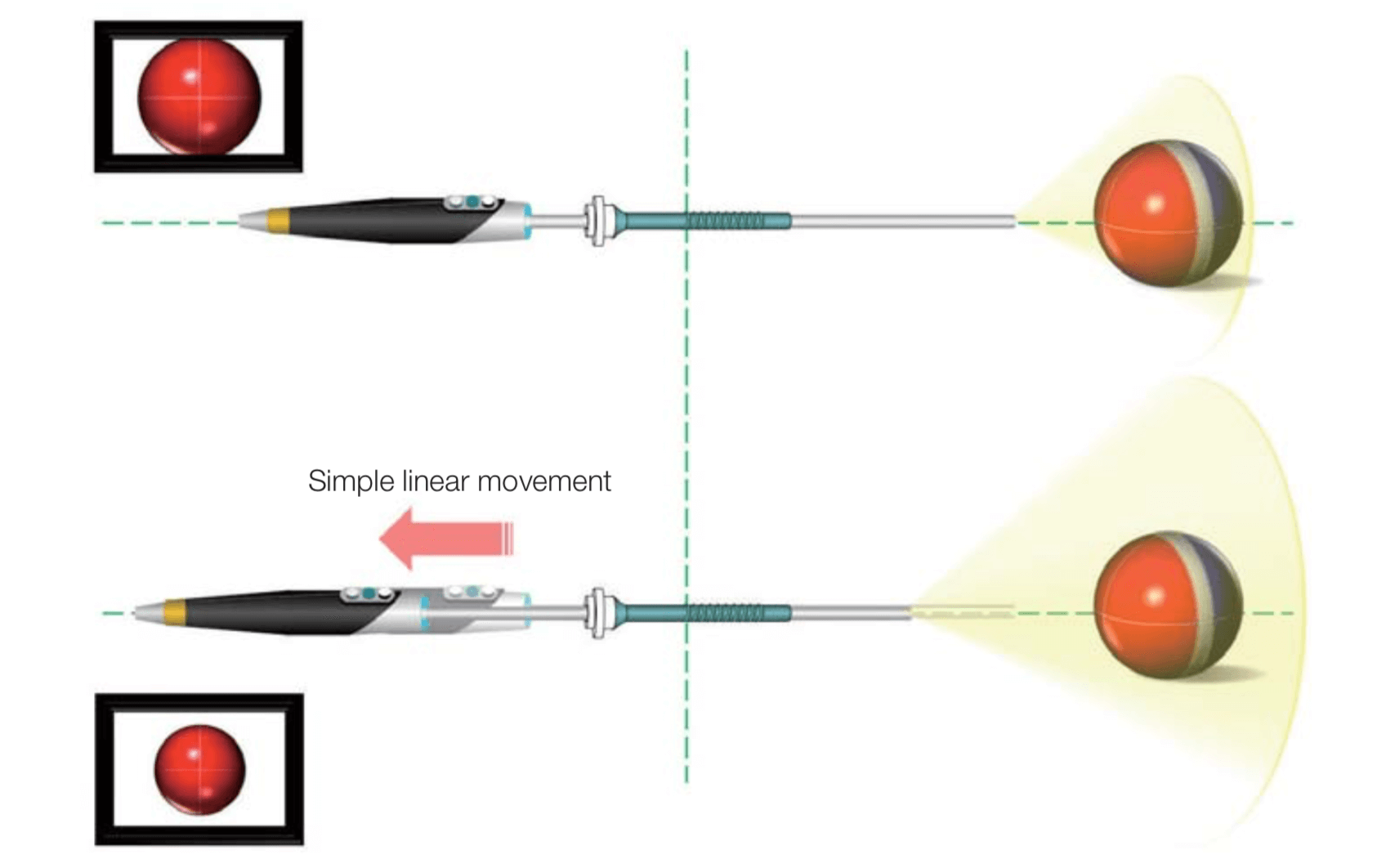
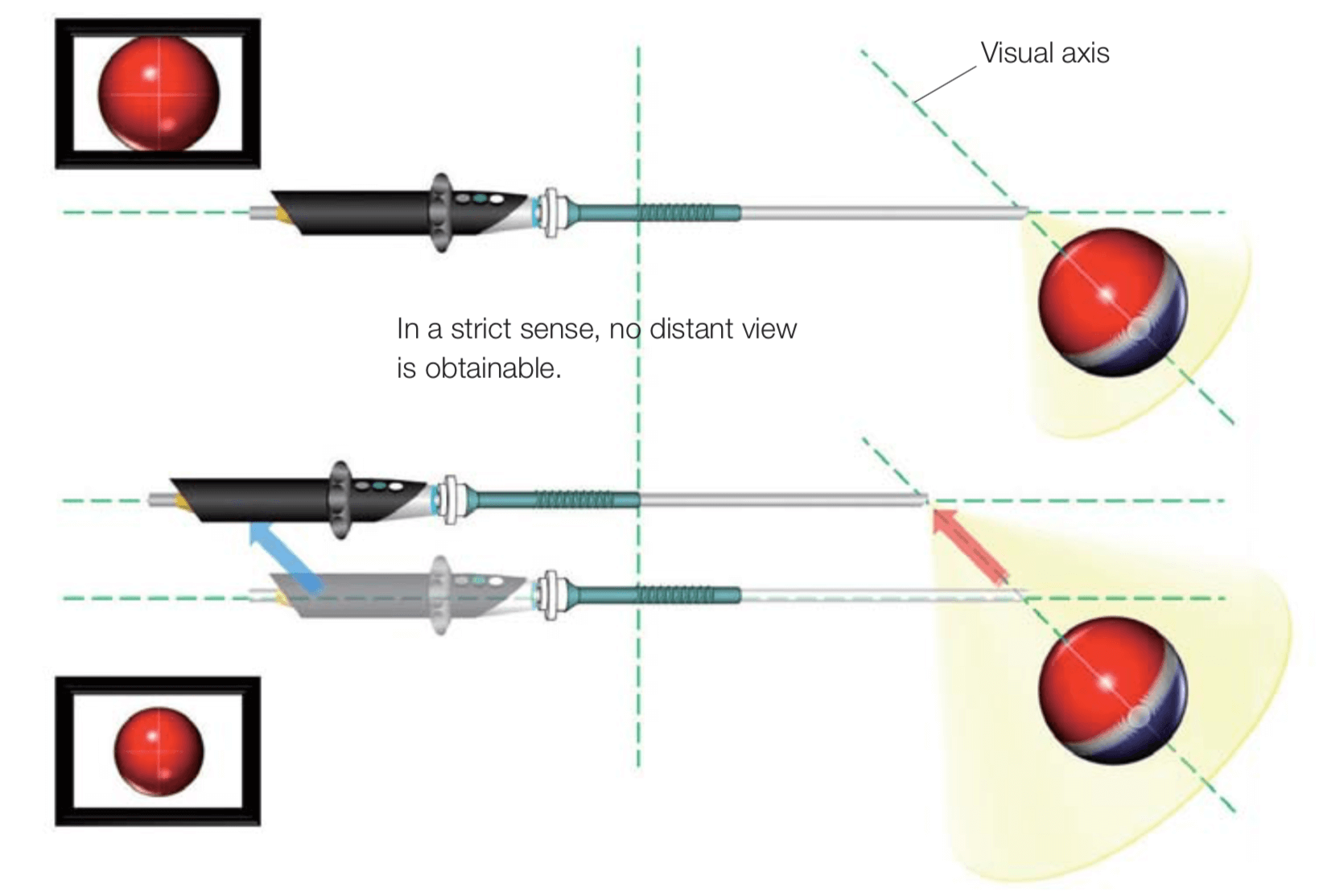
iii Distant view with oblique view rigid laparoscope
With the oblique view rigid laparoscope, a distant view is not obtained when the laparoscope is pulled back in the same way as with the forward view rigid laparoscope, because such operation only causes the object to shift upward in the field of view.
Figure 11 Distant view with oblique view (1)
To obtain a distant view with the oblique view laparoscope as obtained with the forward view laparoscope, it is necessary to pull back the observing point along the visual axis. This operation requires a parallel shift of the laparoscope, which is impossible because the laparoscope is inserted into the trocar to limit the laparoscope movement in this direction.
Figure 12 Distant view with oblique view (2)
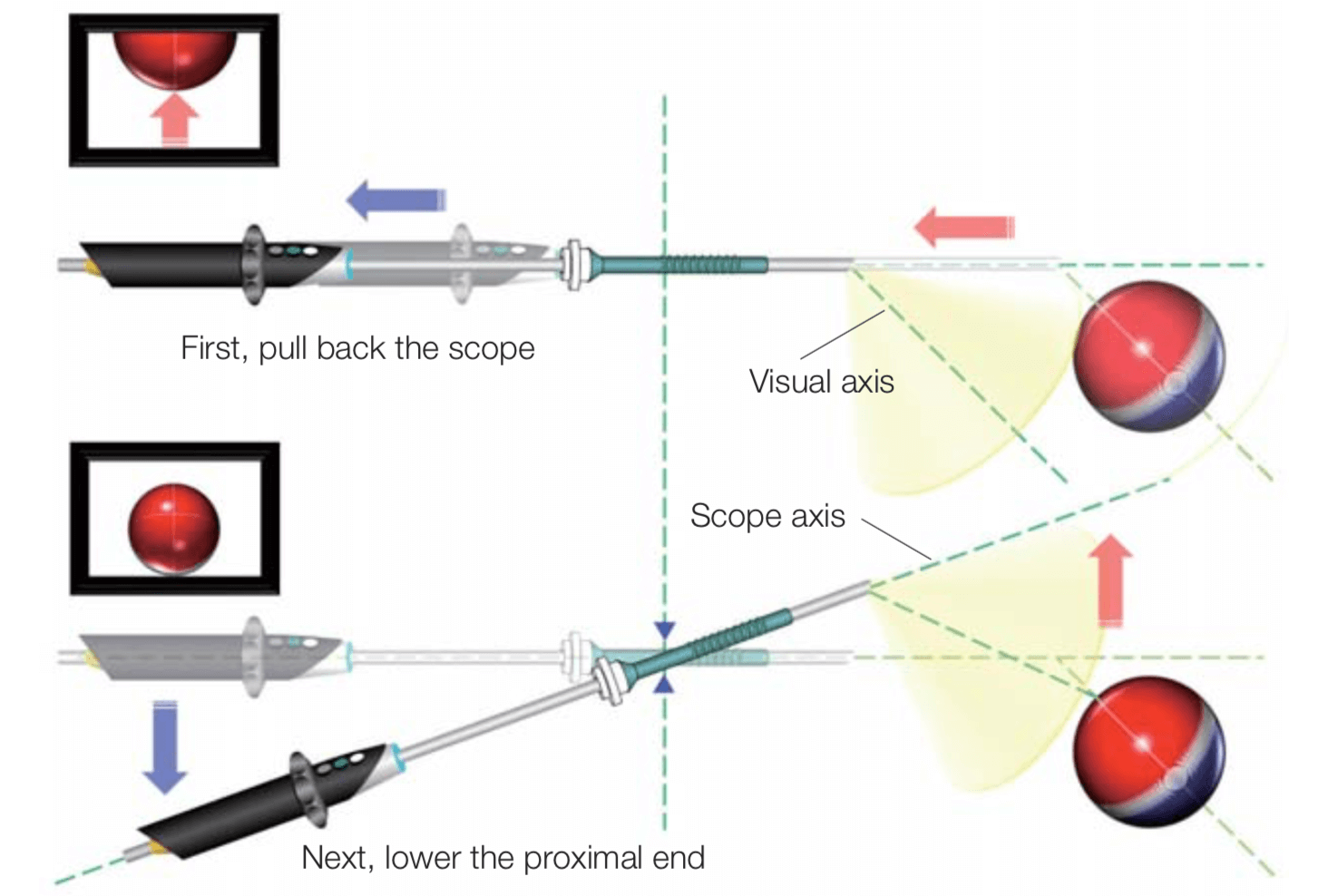
Distant viewing can be obtained with the oblique view laparoscope by pulling back the laparoscope along the scope axis in combination with lowering the proximal end of the laparoscope. This stepwise order of laparoscope operation procedures gives a greatly different view to the surgeon. A surgeon may become irritated to find that the first operative field, obtained when the laparoscope is pulled back, is not a distant view but a view with a parallel shift only. Then the proximal end of the laparoscope needs to be lowered to capture a distant view, which rarely gives an immediate, satisfactory result. This method can be distracting to the surgeon.
Figure 13 Distant view with oblique view (3)
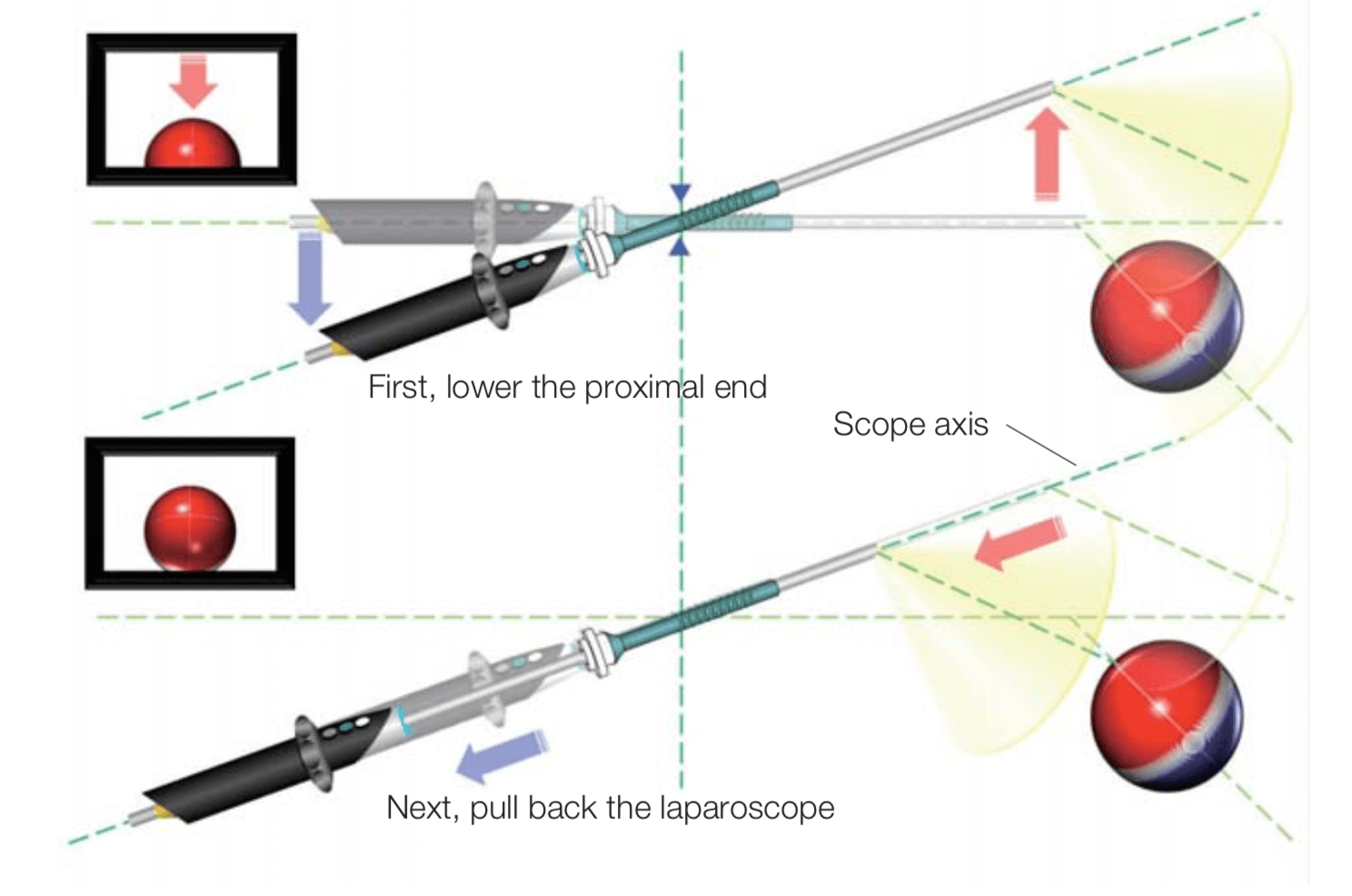
By reversing the steps, the unwanted effects are no longer present. First, by lowering the proximal end to raise the distal end, a wider field of view, which provides a distant view, is obtained on the screen. Second, when the laparoscope is pulled back, a satisfactory distant view is immediately obtained. Similarly, a close-up view can be obtained. Thus, when close-up/distant view operation is tried with the oblique view rigid laparoscope, it is useful to remember the technique: Lower the proximal end first to raise the distal end, and then pull back the laparoscope.
Figure 14 Distant view with oblique view (4)
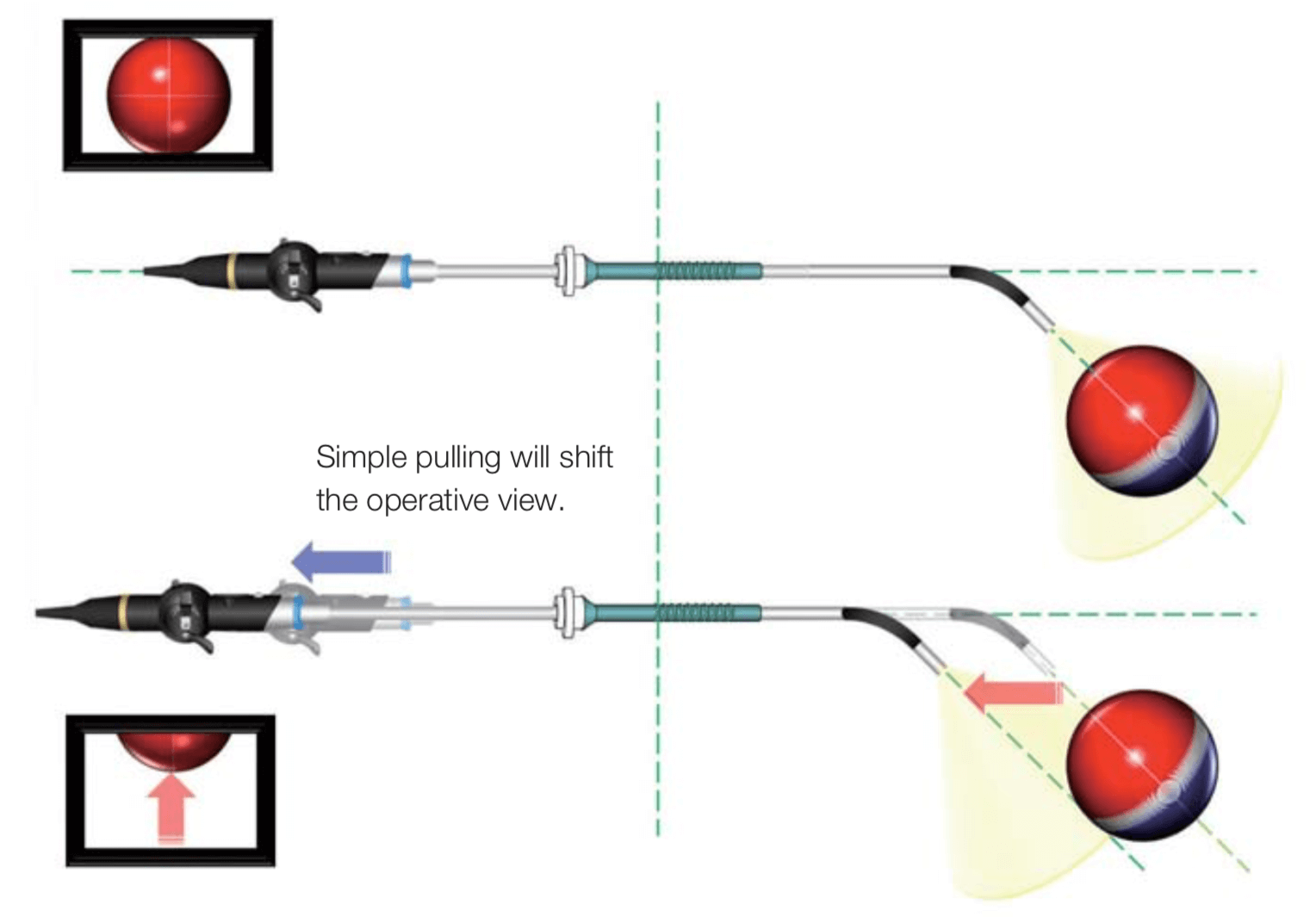
iv Distant view with the ENDOEYE FLEX
The ENDOEYE FLEX provides a distant view image that may not be obtained with the oblique view laparoscope. The same unwanted effect occurs as with the oblique view laparoscope; when the laparoscope is simply pulled back the operative field is shifted.
Figure 15 Distant view with the ENDOEYE FLEX (1)
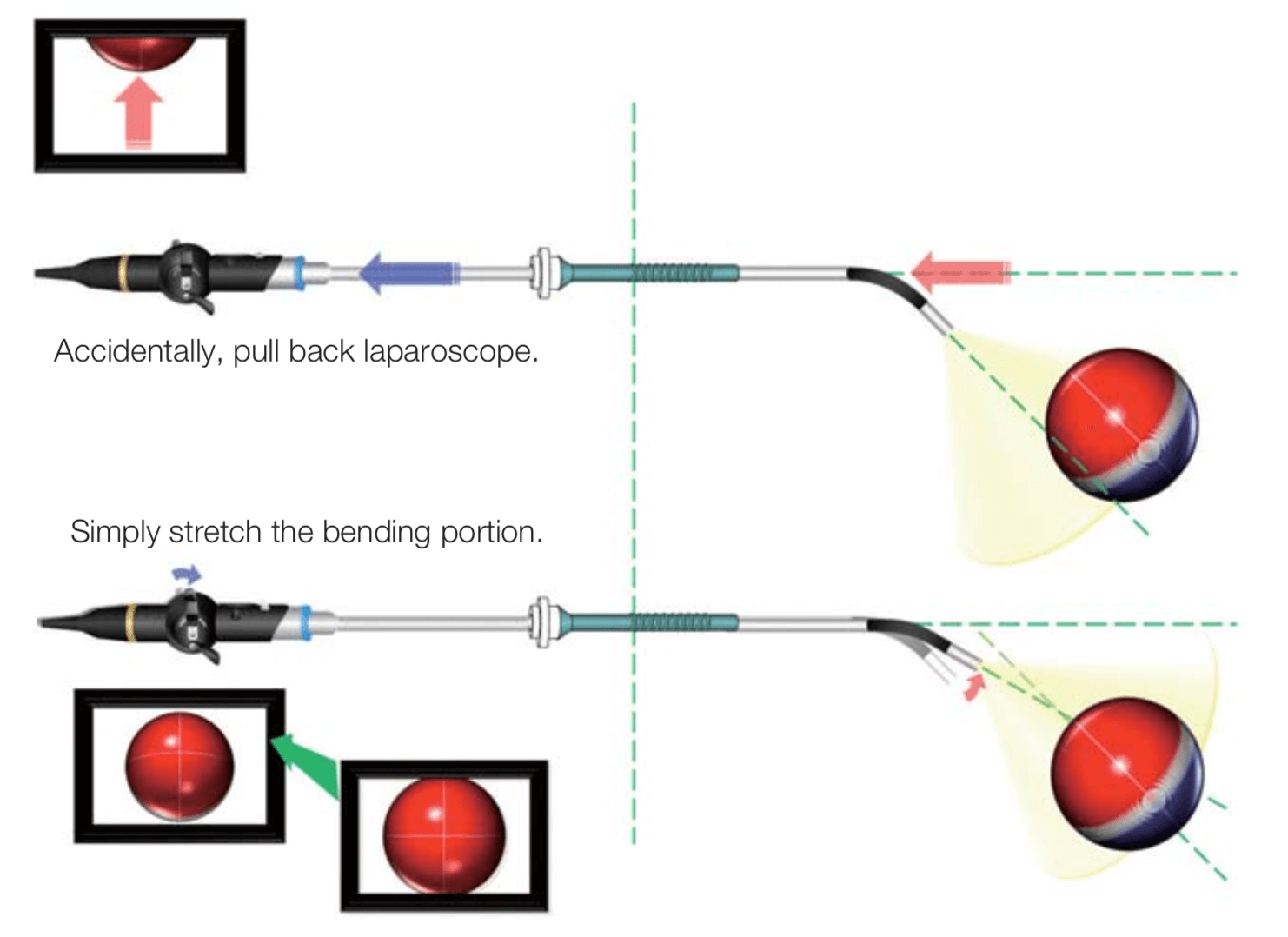
If you have inadvertently pulled back the laparoscope, as with the forward view laparoscope, a distant view may be obtained through operation of upward angulation by stretching the bending section, although there is a slight change in the direction of view. Note, however, that the more the pulling, the more distant the view.
Figure 16 Distant view with the ENDOEYE FLEX (2)
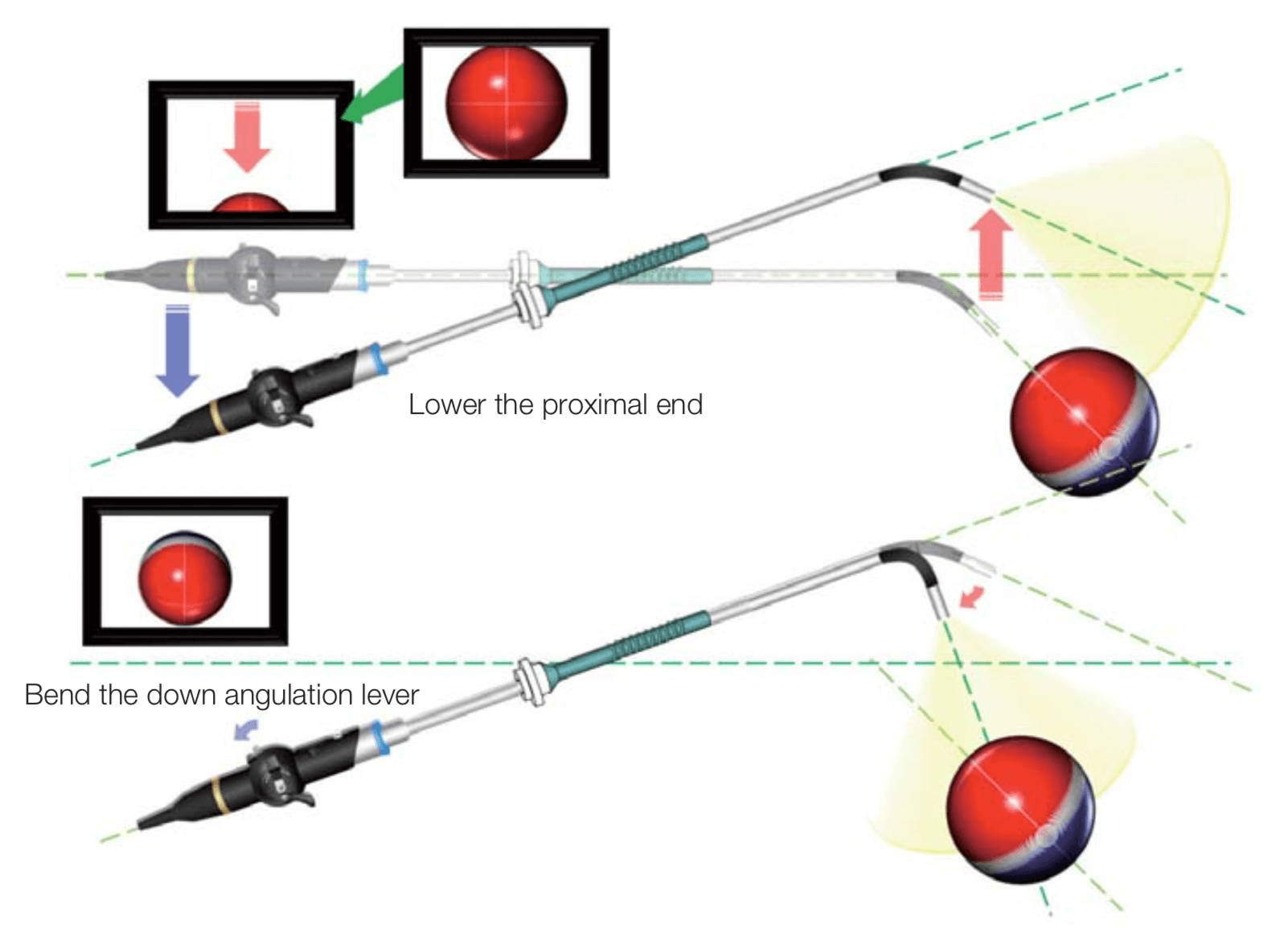
To obtain a satisfactory distant view with the ENDOEYE FLEX, try to move the observing point away from the object by lowering the proximal end of the laparoscope to obtain a wider field of view, as you do with the oblique view laparoscope. Then, change the scope angulation to obtain a distant view instead of pulling the laparoscope along the scope axis to adjust the field of view as with the oblique view laparoscope. With the ENDOEYE FLEX, making full use of the up/down and right/left levers will provide comfortable operability that is not available with rigid laparoscopes. Furthermore, the ENDOEYE FLEX (which requires a compact space for operation) is especially useful for the single-site surgery where the range of the scope handle movement is limited.
Figure 17 Distant view with the ENDOEYE FLEX (3)
- Content Type