Large Balloon with EST
Takao’s Strategy – StoneMasterV

Takao Itoi, MD
Chair and Professor of Department of Gastroenterology and Hepatology,
Tokyo Medical University
EST: The Gateway to Papillary Treatment
At Tokyo Medical University, we regard EST as the first-line treatment for patients suffering from common bile duct stones. Where necessary, papillary treatment can be facilitated by endoscopic techniques such as mechanical lithotripsy (ML) and EPLBD, which is used for the removal of large stones. At our hospital, we apply EST to virtually all cases, with the width of the incision in the medium range (as far as the encircling fold).
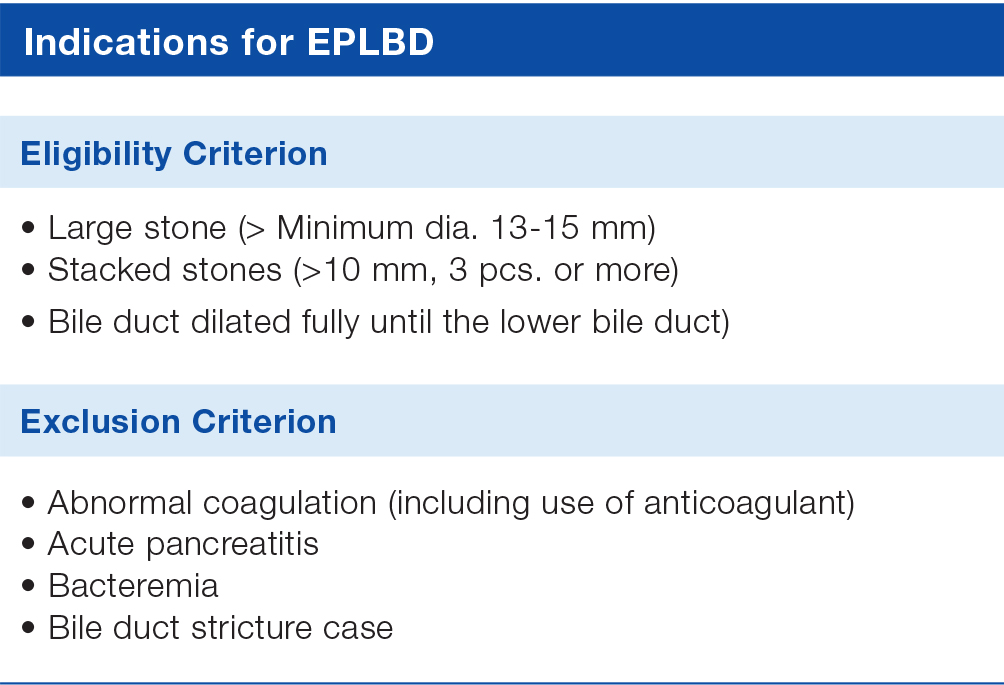
EPLBD is usually indicated for patients with large stones or stacked stones with dilated bile ducts. Basically, EPLBD is applied as an additional treatment when it is determined during papillary treatment that stones cannot be removed with EST alone.
Advantages of Using EPLBD with EST as the Primary Treatment Method
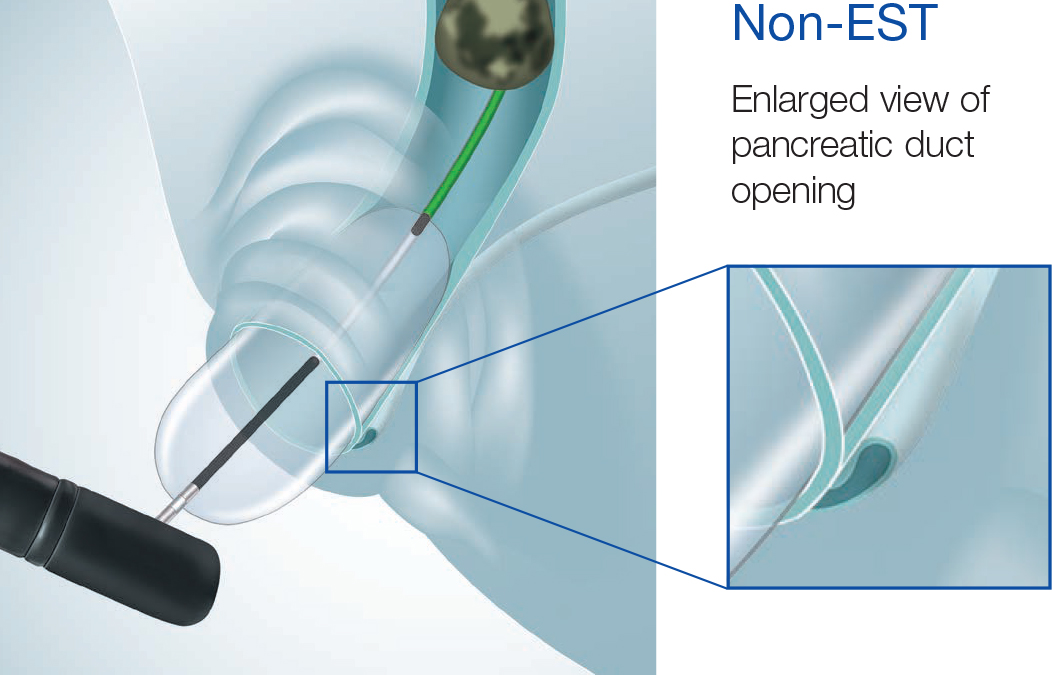
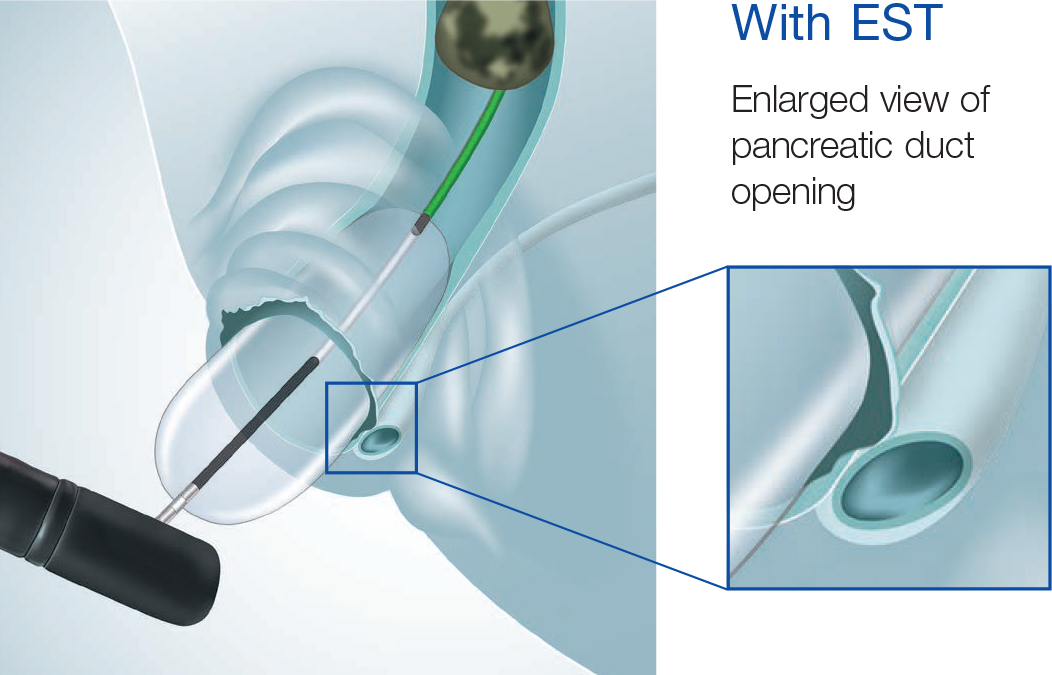
For patients with intact papillae capable of undergoing EPLBD with EST, the advantages are many (low invasion, low cost, etc.). Once MRCP and CT scans have confirmed that the patient is a suitable candidate, we will normally go ahead and perform treatment using EPLBD with EST. The biggest advantage of EPLBD with EST is that it reduces the mechanical compression of the pancreatic duct opening normally caused by the balloon pressure applied to the bile duct when EST is performed. This can be particularly beneficial as we believe it can help reduce the risk of pancreatitis.
Benefits of the Low-pressure Setting on the StoneMasterV
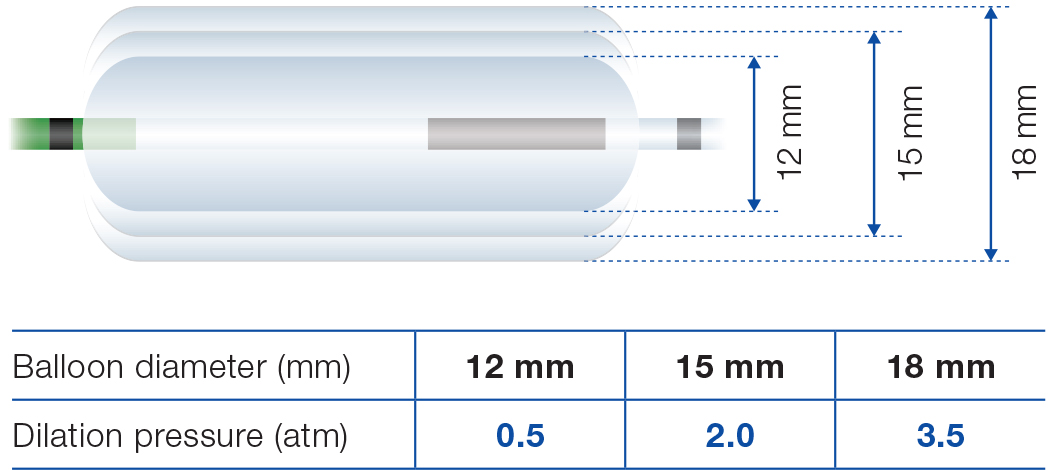
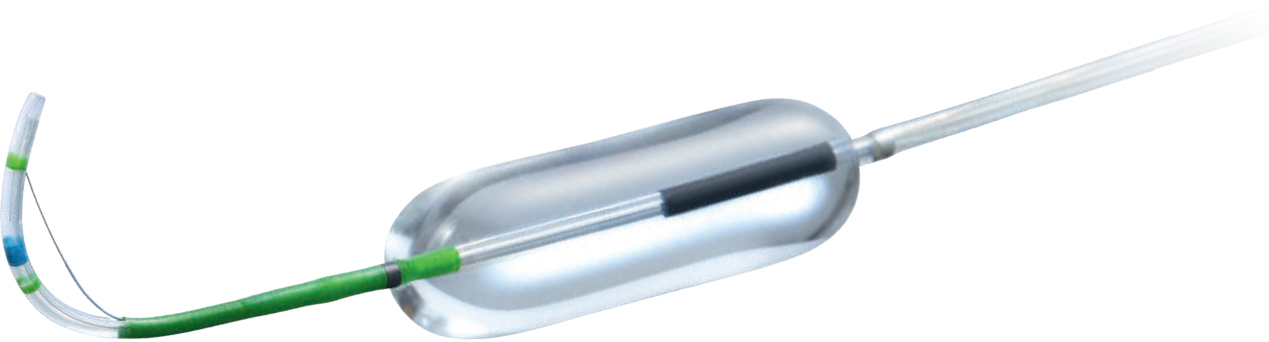
The best way to perform EPLBD is to dilate the duct at low pressure. This helps minimize the loads on and risks to the duodenal papilla and bile duct. In our opinion, the low-pressure setting of the StoneMasterV is best suited for this purpose.
When using StoneMasterV previously, we have always found dilation to be more than adequate and have never experienced any problems when performing a procedure. We also believe that low-pressure dilation even with a large-size 18 mm-diameter balloon can support safer EPLBD procedures.
Effective Use of Convenient “C-hook” Tool

The coexistence of the knife and balloon functions sometimes makes the inflator and knife control section bulky during dilation. In this case, we recommend securing the knife control section to the scope using the C-hook. The C-hook can also be useful with Olympus products other than StoneMasterV, especially in situations where not enough assistants are available.
Selection of Balloon Size in EPLBD
Our policy when selecting a balloon size is to select a balloon with a maximum dilation diameter one step larger than the expected bile duct diameter. This means that in EPLBD using the separate type we typically select a balloon with a diameter between 15 and 18 mm. The reason we select a balloon slightly larger than the target bile duct is that this allows us to dilate the duct without reaching the maximum dilation pressure of the balloon, making possible safe dilation under low pressure. Even if the selected balloon does not reach the bile duct diameter, it is still possible to take advantage of the “dilating margin”, which enables additional dilation. We have also found that having some margin can reduce the load to the papilla and better facilitate stone removal than when using a balloon that fits exactly. Further to this, we believe that selecting the maximum dilation diameter of the balloon does not lead to any increased risk of complications. If this is the case, then going by the maxim, “the bigger, the better”, would make perfect sense. Using a larger balloon that doesn’t have to be maximally dilated may lead to safer EPLDB procedures than increasing the pressure of a small-diameter balloon to the maximum.
EPLBD (Dilating margin)
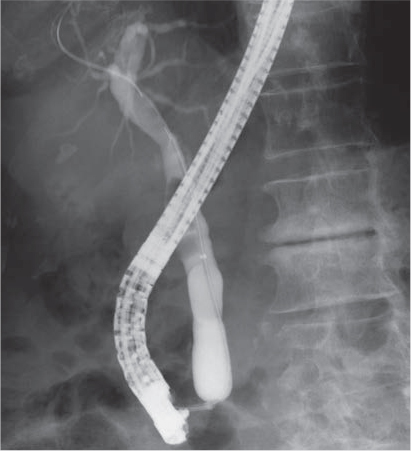

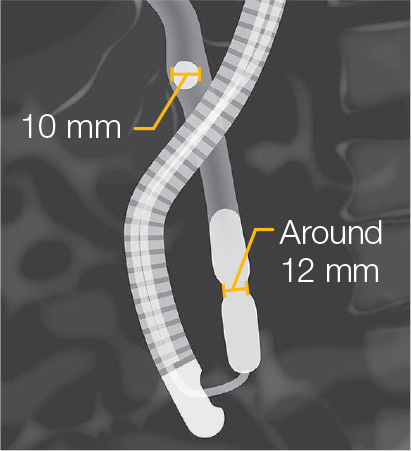
Treatment of the papillary sphincter does not require dilation greater than the stone size. Instead, low pressure can be safely used by controlling the dilation at the minimum necessary level. The StoneMasterV has a maximum dilation diameter of 18 mm, but we believe that a diameter of 12 to 15 mm is sufficient with stones no larger than 12 mm.
Safe Use of EST Knife Inside the Bile Duct
Because the StoneMasterV has been designed to allow the operator to proceed directly to EPLBD after EST, some doctors have expressed concern about the potential risks associated with insertion of the knife into the bile duct. We are confident that this design in no way compromises safety; rather, we believe that deep insertion of the device with wire-guided cannulation actually makes dilation safer because the balloon is stabilized near the papilla and cause no significant position deviation during EPLBD.
- Content Type