Retrieval Balloon
Hiroyuki’s Strategy – Multi-3V Plus™ device

Hiroyuki Isayama, MD
Professor, Department of Gastroenterology,
Graduate School of Medicine,
Juntendo University
Dr. Hiroyuki Isayama, MD is a paid consultant of the Olympus Corporation, its subsidiaries and/or its affiliates.
Any claims and/or comparisons within this article are solely the opinion of Dr. Hiroyuki Isayama, MD.
Any content or information (“Content”) presented herein is illustrative in nature and does not guarantee or represent specific information, outcomes or results.
Under no circumstances shall Olympus or its employees, consultants, agents or representatives be liable for any costs, expenses, losses, claims, liabilities, or other damages (whether direct, indirect, special, incidental, consequential, or otherwise) that may arise from, or be incurred in connection with, the Content or any use thereof.
Olympus Corporation of the Americas and its parents, subsidiaries, affiliates, directors, officers, employees, agents, and representatives (collectively “Olympus”) do not represent to or warrant the accuracy, reliability or applicability of the Content.
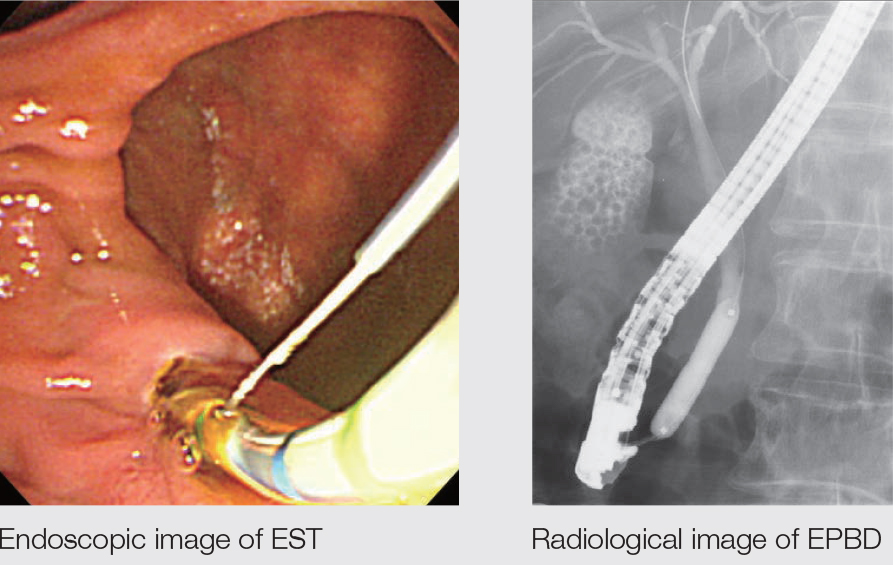
EST Small Incision + EPBD is the Basic Policy
Our basic policy in dealing with stones is to perform the EST small incision + balloon dilation. We use the EPBD balloon for stones from 8 to 10 mm, and perform EPLBD, if possible, with stones of 12 mm or more. EPBD only is used with patients taking an oral antithrombotic, patients with abnormal blood coagulation due to hepatic diseases, patients subject to hepatic ablation, patients with benign biliary hilar stricture, etc. This is because eliminating the papillary functions with the EST brings about the risk of hepatic abscesses in the regions exposed to radio waves or areas without drainage. We also attempt EPBD in cases where EST is difficult and/or risky – for example, with patients with postoperative reconstructed gastrointestinal anatomy.
Advantages of Small Incision + Balloon Dilation
One of the main advantages of the EST small incision and additional balloon dilation technique is that no special skills are required so they can easily be performed by even non-expert endoscopist. We also believe that stone removal is easier with this technique than with EST alone or EPBD alone because it can open up the papilla sufficiently. We see it as a technique that boasts many advantages, including a low probability of complications such as perforation, bleeding and pancreatitis. Overall, the simplicity of the technique combined with a lower risk of mistakes makes this an excellent choice for papillary treatment with high safety and low risk – factors which, we believe, are critical to success. When we perform EPLBD, we usually add EST as well. However, even without EST, both efficacy and safety are first class, so we are comfortable performing EPLBD even with cases where EST is difficult.
If the diameter of a stone is larger than the dilated diameter of the EPLBD, we select the lithotripsy basket considering the risk of impaction. We recommend that retrieval without crushing the stone should be tried first. Only crush the stone if it is too difficult to retrieve it otherwise.
EST + EPBD
Choosing a Stone Extraction Device
The first criterion for selection is whether there is a possibility that it will be necessary to crush the stone. If there is not, select the balloon. If the stone is big enough that there is a risk of impaction, select the lithotripsy basket.
When we used to perform EPBD almost exclusively, the insufficient opening of the papilla made it necessary to select a basket that could catch and remove the stones. This was also the same when only EST was performed. However, with the introduction of small incision + balloon dilation technique, opening the papilla was no longer a problem, so the strategy has changed because extraction using a balloon is easy. Stone extraction using a balloon is simple, and that is one of the main advantages of this technique.
We believe that the basket is most effective in those cases where there is a pocket at the lower end of the bile duct. In these cases, or when there is a small papillary opening, it is necessary to catch the stones securely with a basket for extraction. The most important thing to remember is that the stone extraction device should be selected according to the degree of opening of the papilla.
Selecting a Balloon
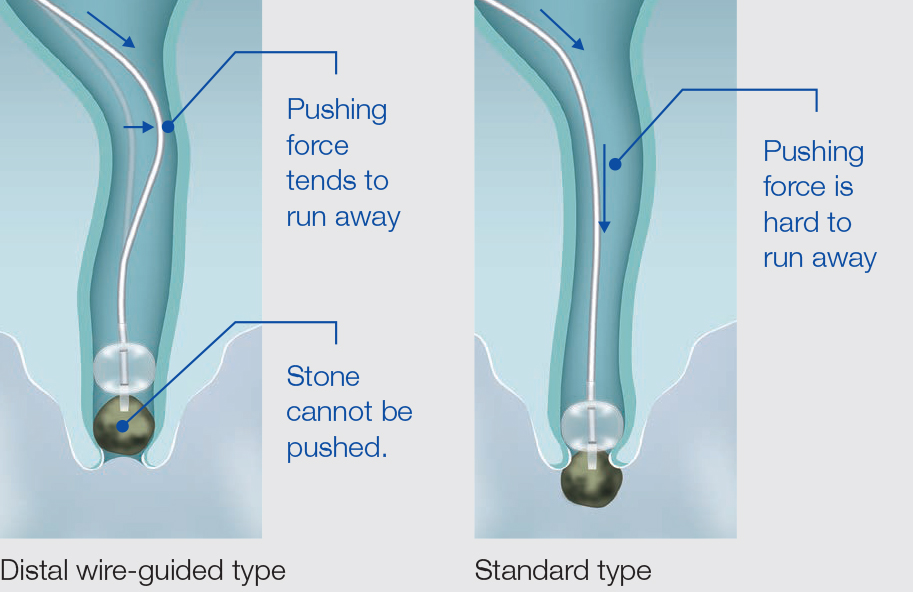
There are a surprisingly large number of balloon types classified for very specific applications, including the position of the injection port, the position of guide wire passage, and the size of the balloon. When choosing between the standard (over-the-wire) type and distal wire-guided type, we generally use the distal wire-guided type because of its high degree of usability. We find the standard type effective in cases where pushability is required – for example, when the stones are pushed through the HGS route.
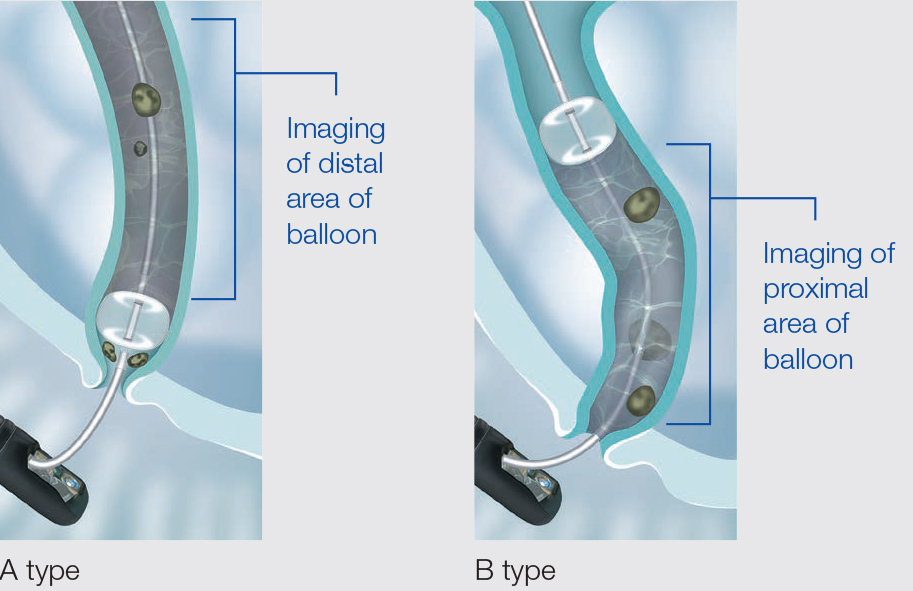
We also choose the standard type if the operator is a trainee, as well as providing support for the procedure. For the injection port, our favorite choice is the type with an opening on the distal end (A-type). This type makes it easy to check for residual stones and to prevent small stones from slipping through the sides of the balloon. This may occur when the pressure in the region on the intrahepatic side of the balloon becomes negative during extraction. This can be avoided by setting the pressure on the intrahepatic side to positive using the A-type port
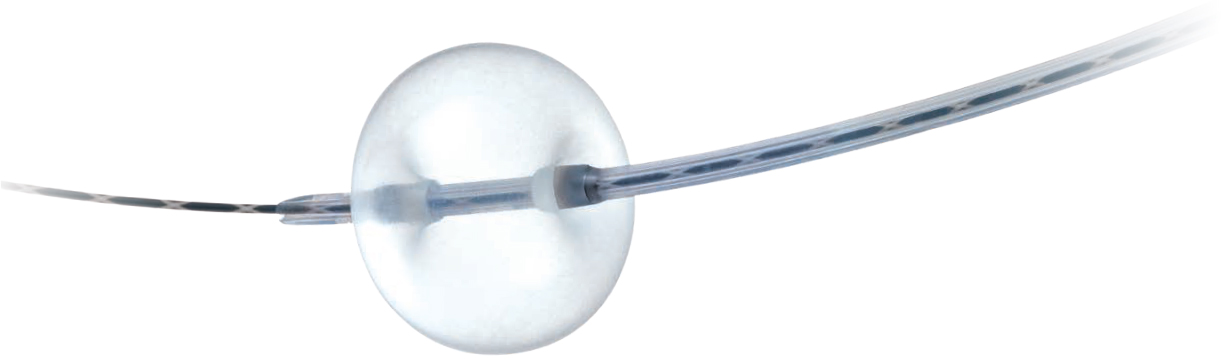
Safe Balloon Use
The balloon size should be selected to match the bile duct diameter. When removing stones from a narrow location – for example, with stones presenting proximal to the common hepatic duct – it is necessary to take care to avoid excessive balloon inflation. If there is an aberrant small stone inside the liver, it should not be swept out by force with the balloon. Instead, the technique we find most useful is to inflate the balloon inside the common bile duct to sweep the stone out with negative pressure. Olympus balloons are equipped with radiopaque bands at the distal and proximal ends of balloon. This is beneficial because they facilitate confirmation of the position where the inflation begins. Ideally the balloon’s shape should extend laterally rather than longitudinally. Longitudinal extension may cause interference with stones, while the lateral extension facilitates clearance of the stones. From this perspective, the laterally extending design of the Multi-3V Plus™ device is effective. It can also be recommended because there is very little deviation or deformation of the balloon caused by friction inside the bile duct.


A Tip on Deflation
Deflation adjustment on the Multi-3V Plus™ device is relatively easy.
When fine deflation control is necessary, it is often recommended to turn the stopcock by one turn per step, but we recommend the method of supporting the syringe with a palm (palm technique). One of the advantages of this technique is that controlling deflation with the syringe lets the operator sense when the balloon is contacting the wall, making it easier to know when optimum dilation size has been achieved.


Coexistence of Approaching Performance and Operability
There are basically not many cases of use but, if the guidewire slips out after several approaches, we feel that the bile duct approach using the balloon can be continued because Multi-3V Plus™ device maintains the effective cannulation performance. We believe that the variation of catheter diameters on the distal and proximal ends makes it possible to provide both the effective performance and operability.
* All images are Olympus owned unless otherwise indicated
Olympus is a registered trademark of Olympus Corporation, Olympus America Inc., and/or their affiliates.
- Content Type