Non-muscle-invasive bladder cancer
Case 1 pTA LMP Male, aged 76
History
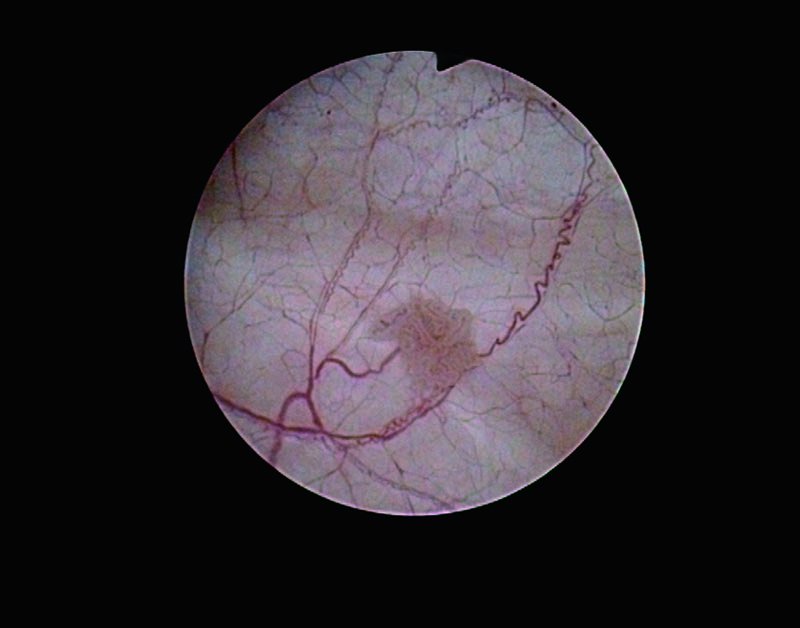
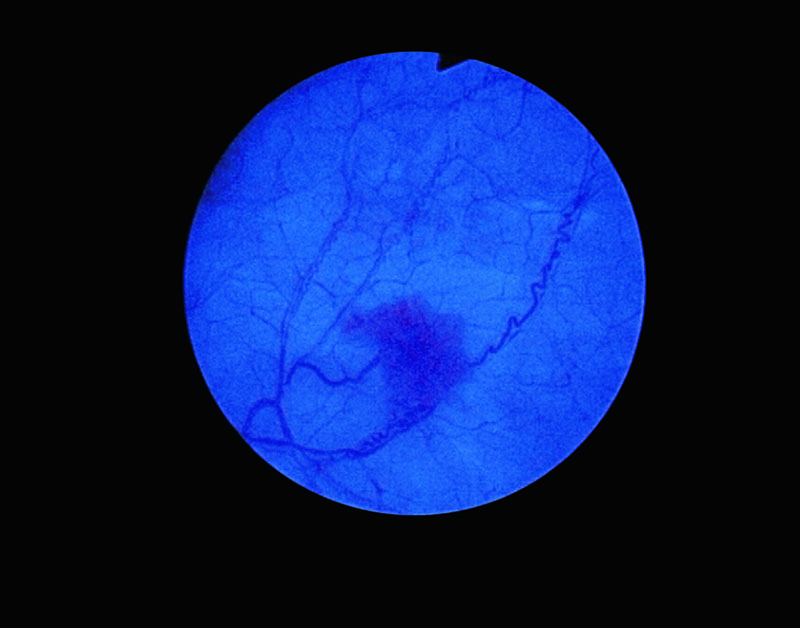
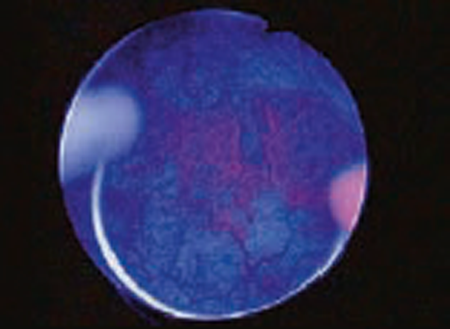
76 yo male, fi rst cystoscopy for gross haematuria shows two small (5 mm) papillary lesions that are faintly fluorescent. Washout cytology is not indicative of of urothelial carcinoma.
Pathology
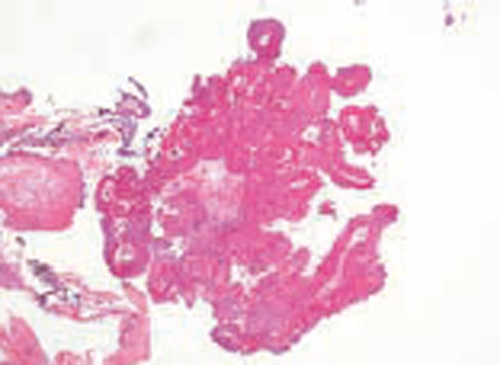
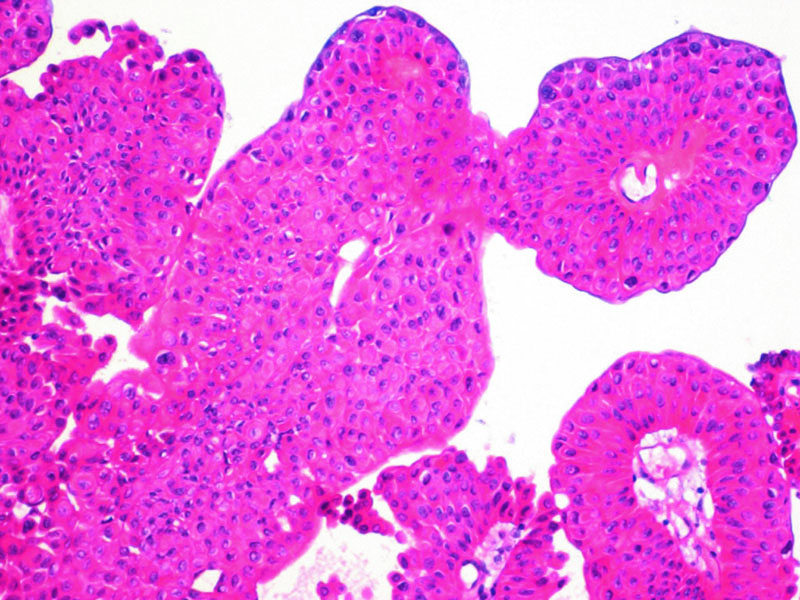
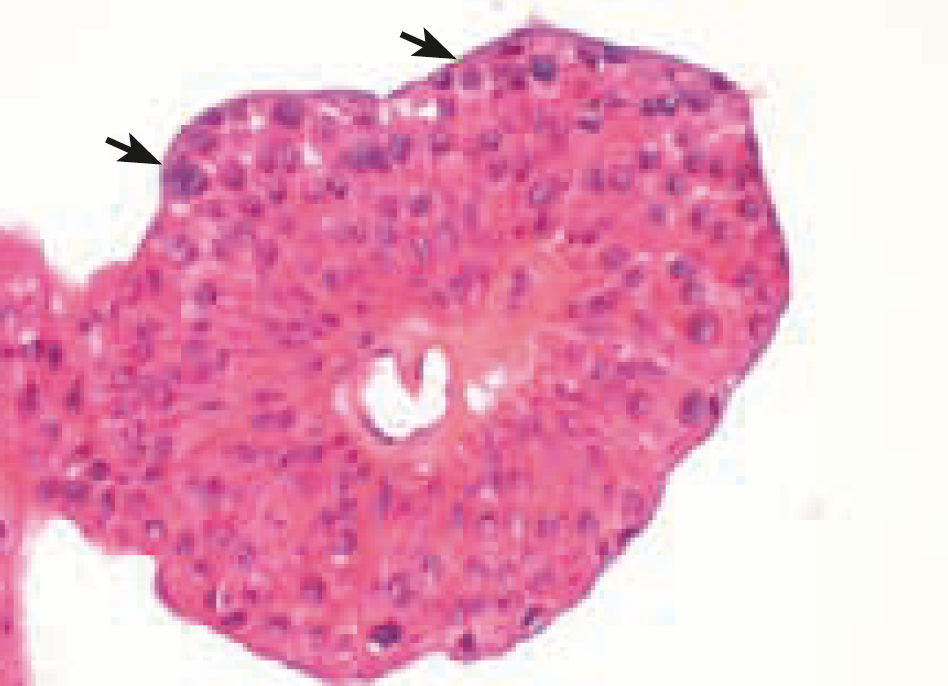
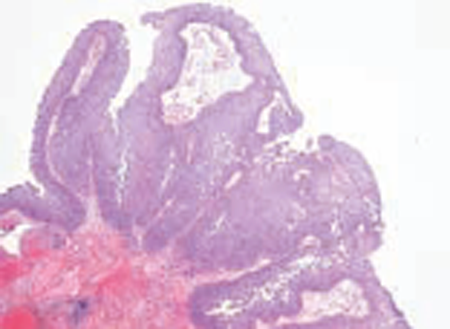
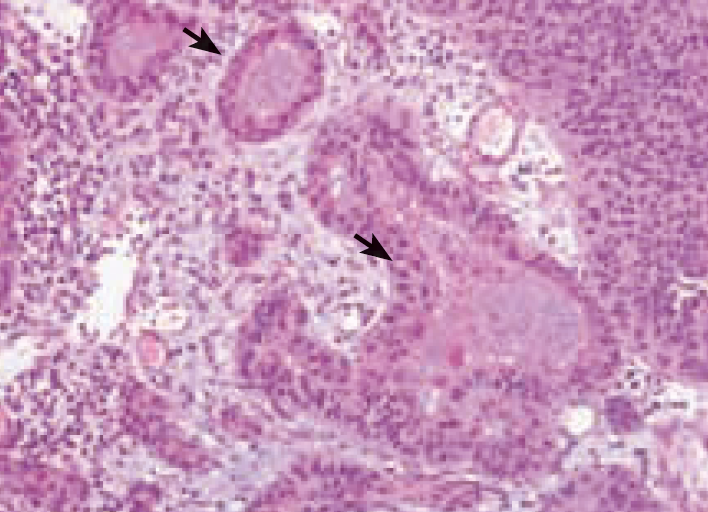
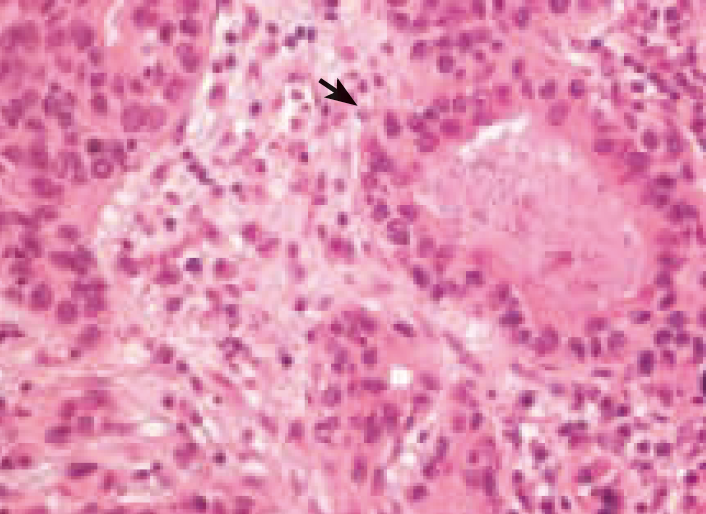
This tumour shows discrete and not fused papillary stalks that are covered by a multilayered urothelium with minimal atypia. Note the presence of terminally differentiated umbrella cells (arrowhead) and the absence of mitotic figures.
Case 2 pTA LG

History
First diagnosis of pT1aLG one year before followed by eight cycles of MMC. First recurrence eight months later (pTaLG with small foci of pTaHG (10%) treated by BCGx6). Present follow-up cystoscopy shows multiple areas of papillary lesions with indiscriminate borders that are faintly fluorescent. Cytology was not evocative of HG tumour.
Pathology
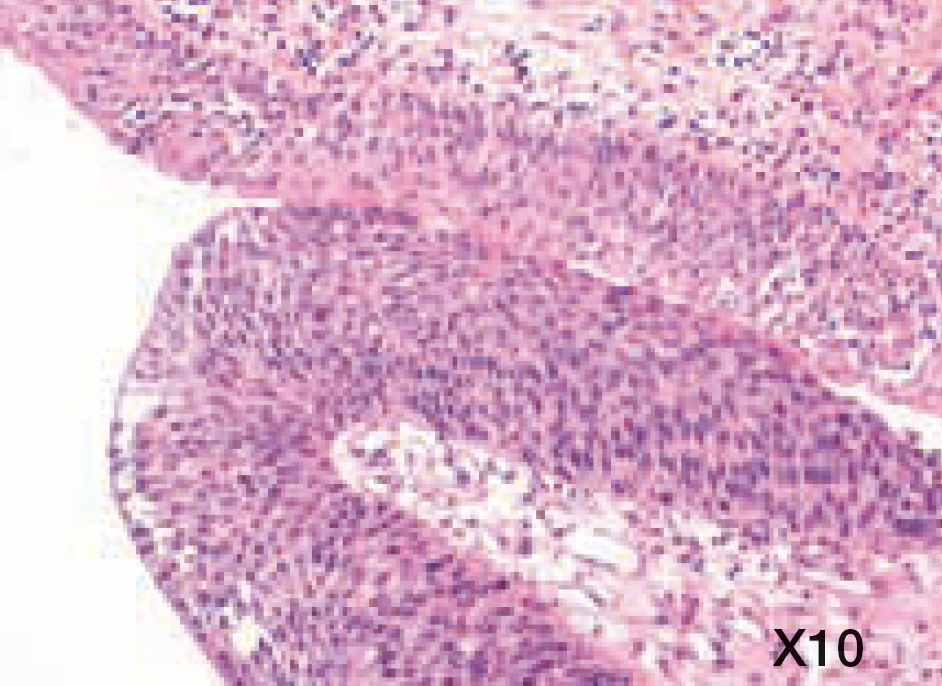
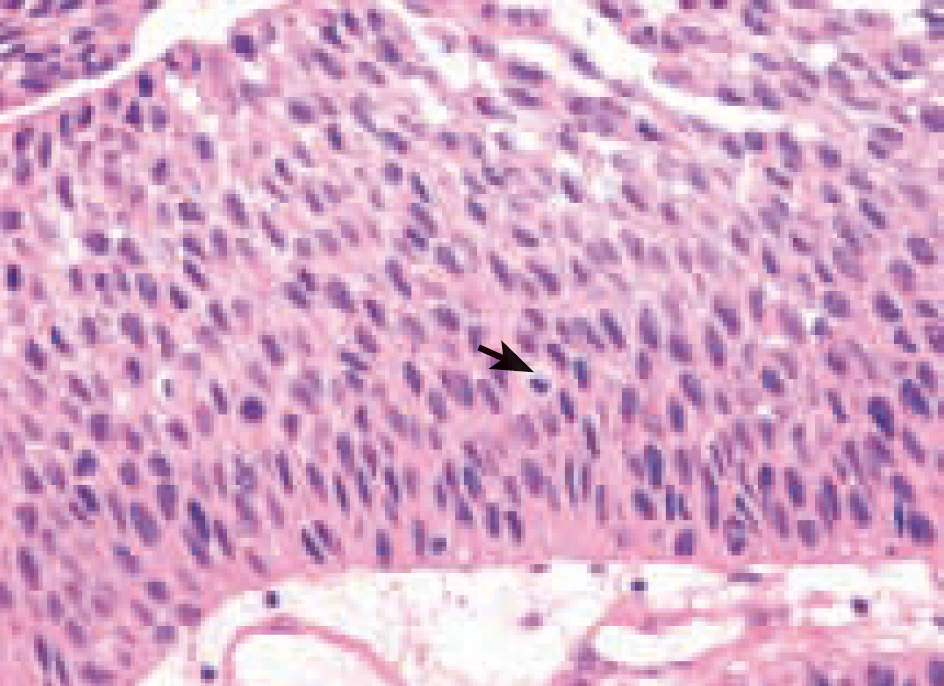
Coalescent papillary stalks with orderly but variable (x10 power) organisation of the urothelium layer that benefits the WHO 2004 definition of low-grade tumour (WHO 1973 grade I). Note one mitose (arrowhead) that is not located in the basal layer.
Case 3 pTA HG Male, aged 53

History
First diagnosis of pT1aLG one year before followed by eight cycles of MMC. First recurrence eight months later (pTaLG with small foci of pTaHG (10%) treated by BCGx6). Present follow-up cystoscopy shows multiple areas of papillary lesions with indiscriminate borders that are faintly fluorescent. Cytology was not evocative of HG tumour.
Pathology
Coalescent papillary stalks with orderly but variable (x10 power) organisation of the urothelium layer that benefits the WHO 2004 definition of low-grade tumour (WHO 1973 grade I). Note one mitose (arrowhead) that is not located in the basal layer.
Case 4 pTI HG Male, aged 53
History
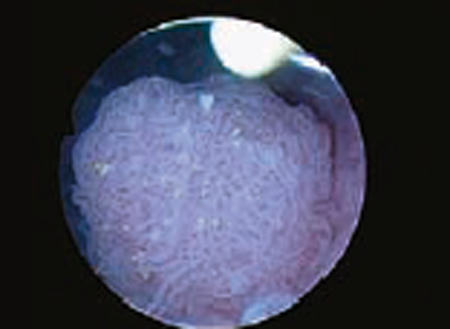
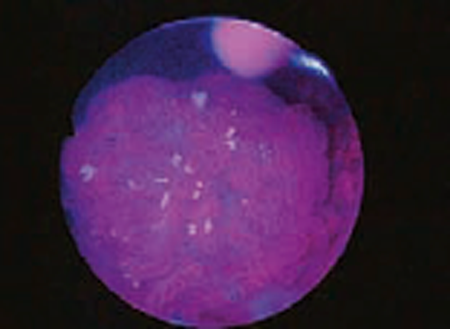
53 yo male, non-smoking, first cystoscopy for gross haematuria shows a massive (3 cm wide) and intensely fluorescent tumour in the bladder base, with two flat lesions in the vicinity that proved to be CIS.
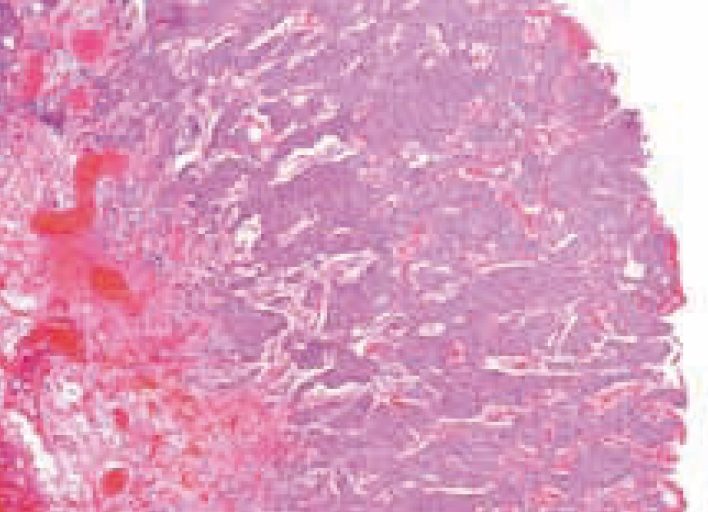
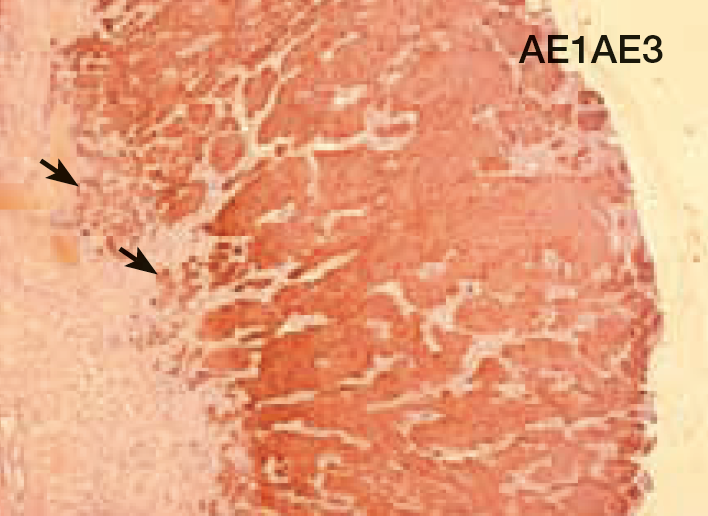
Pathology
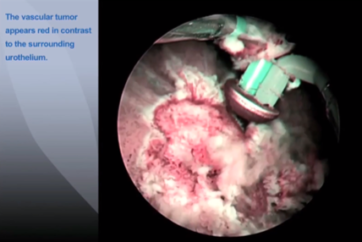
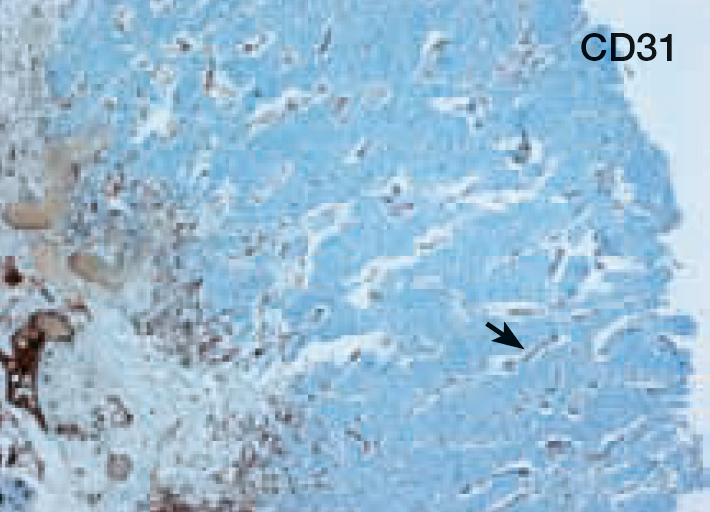
Massive and coalescent papillae with invasion of the superficial stromal layer by high-grade carcinoma, as shown by anti-cytokeratin immunostaining (AE1AE3). Note the high microvessel density, evident on H&E staining and confirmed by anti-CD31 staining.
Case 5 pTI HG Male, aged 81

History
81 yo male, previous history of recurrent “superficial cancer” in another centre. Cystoscopy shows two papillary lesions on the right aspect of the bladder wall with a large (5 cm wide) fluorescent flat lesion on the bladder dome that proved to be CIS. Cytology was inconclusive due to associated inflammatory cells.
Pathology
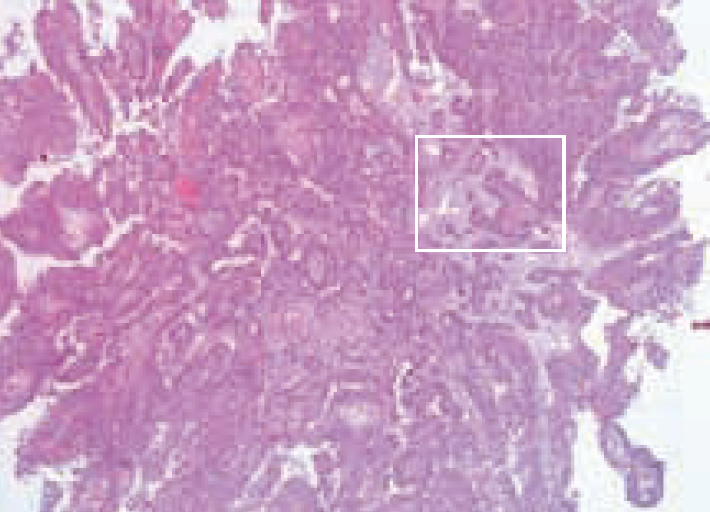
Despite thin and well-formed papillary stalks, invasion of the superfi cial stromal layer is evident on HE staining (box).
High power shows obvious cell atypias with marked pleiomorphism and hyperchromasia. The infiltrative component exhibits a rare microcystic variant with well-formed cysts (arrowhead).
Case 4 (continued) CIS Male, aged 53


History
Discrete area that is slightly raised and intensely fluorescent in the vicinity of a single exophytic high-grade lesion (pT1HG).
Pathology
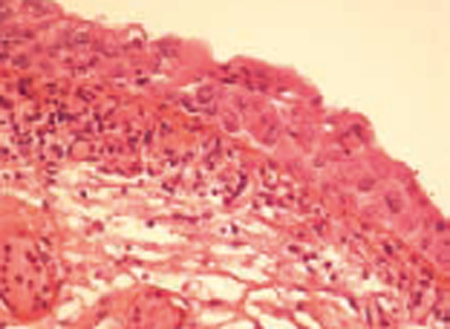
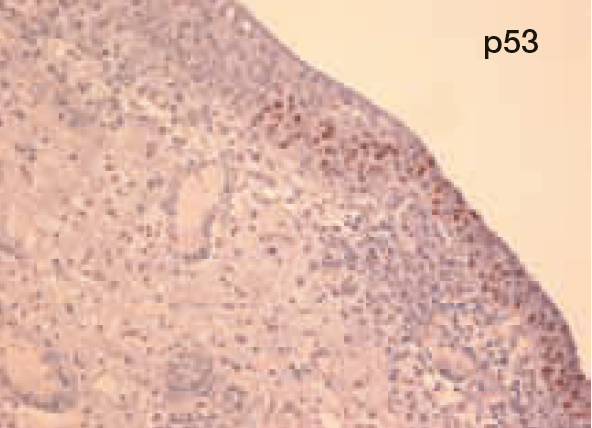
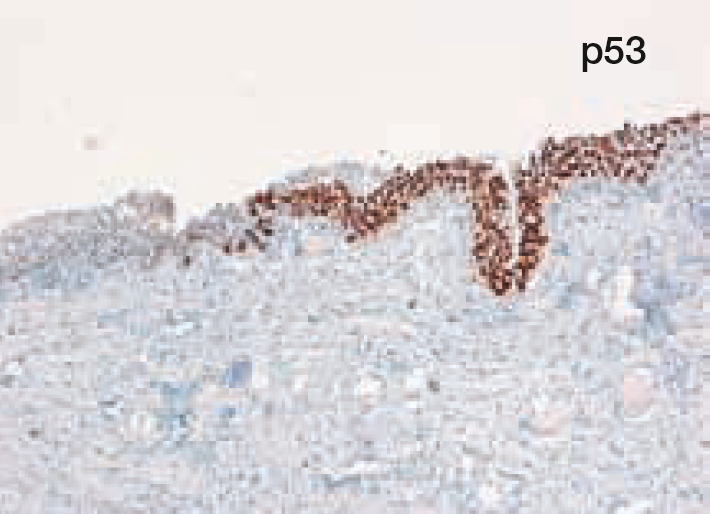
Pleiomorphic cells with hyperchromatic nuclei are found underneath the most superficial layer of the mucosa that retains terminal differentiation (arrowhead) as reported in Amin’s classifi cation (AmJSurg Pathol 2001) as an “undermining” variant of carcinoma in situ. Note intense p53 staining in this contingent.
Case 5 (continued) CIS Male, aged 81
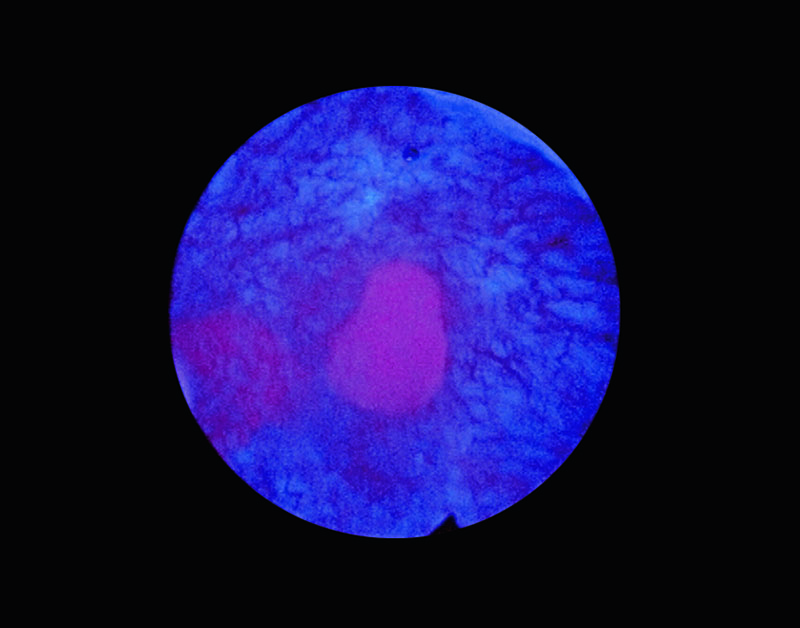
History
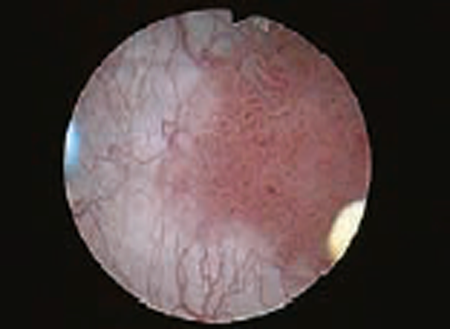
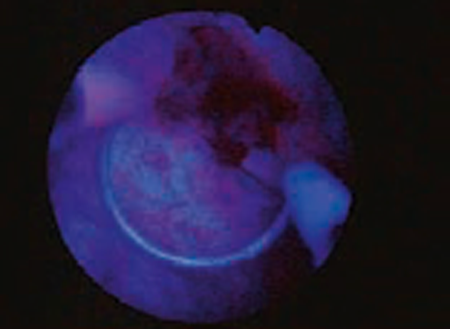
A slightly uneven surface in white light cystoscopy that was intensely fluorescent in blue light was collected by cold-cup biopsy.
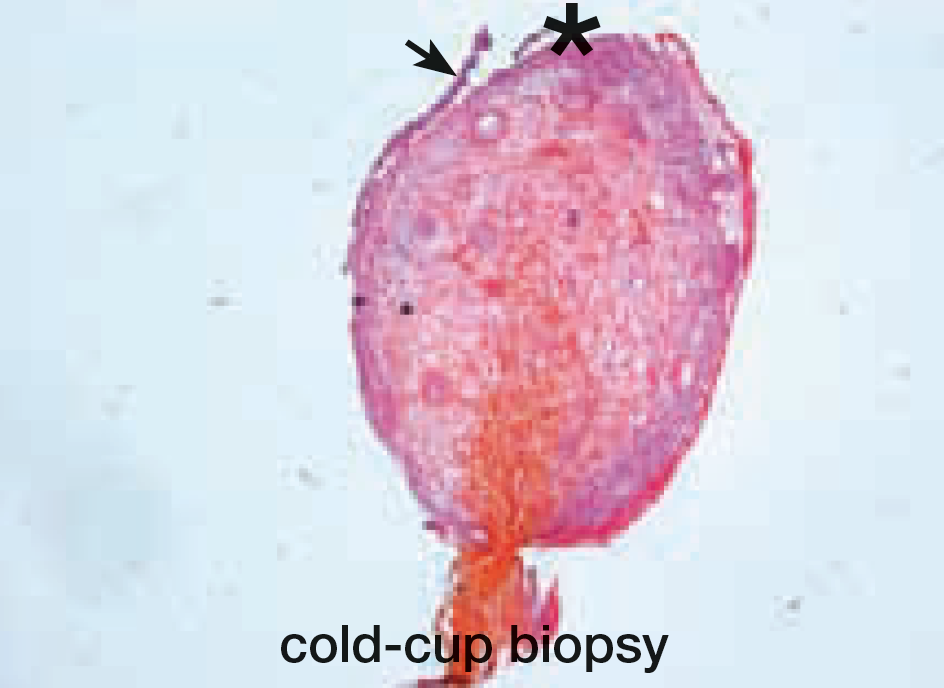
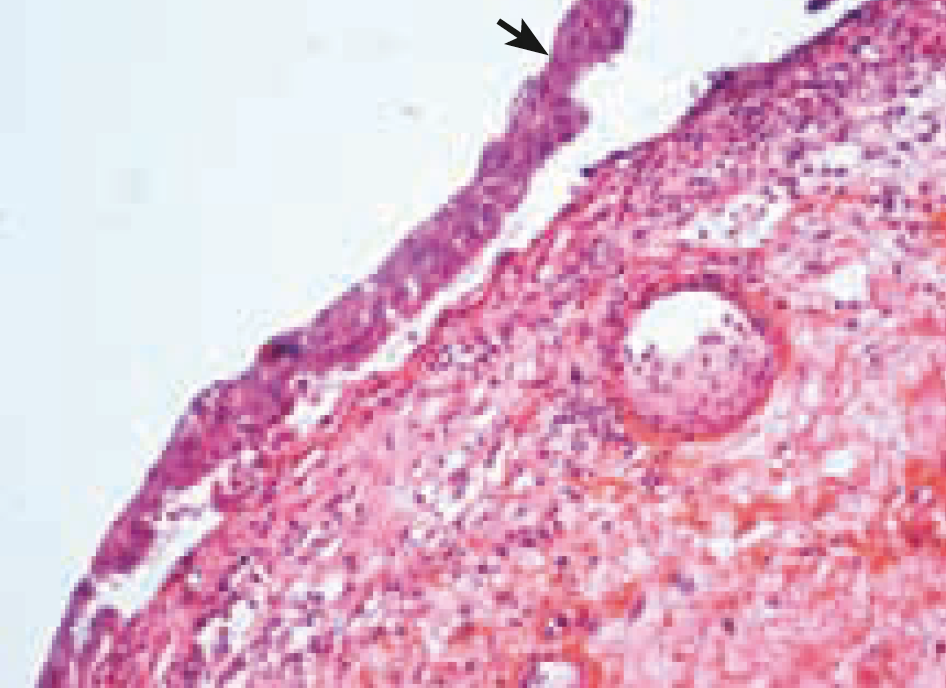
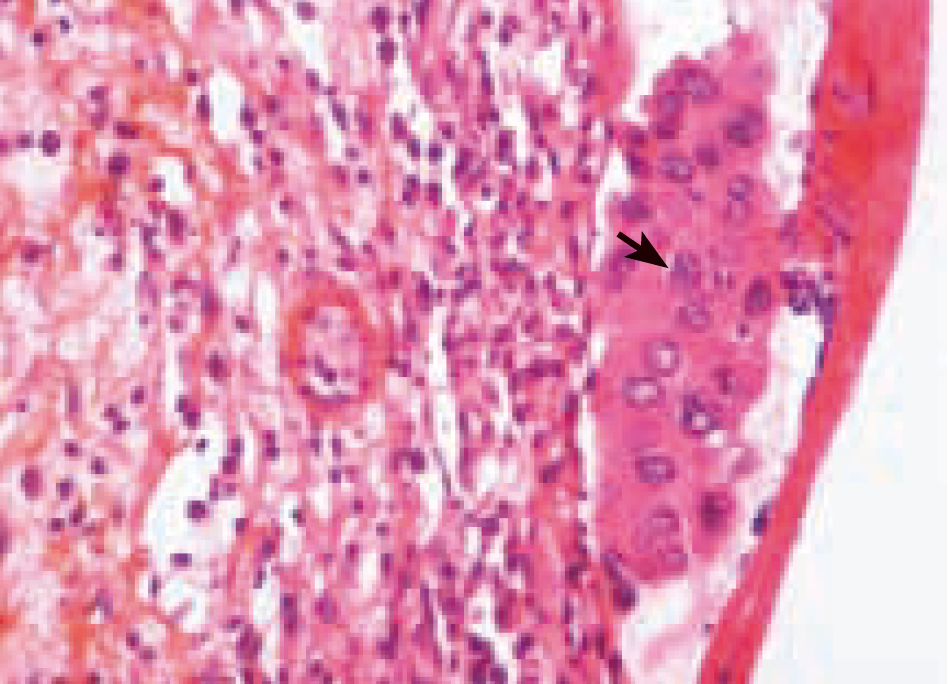
Pathology
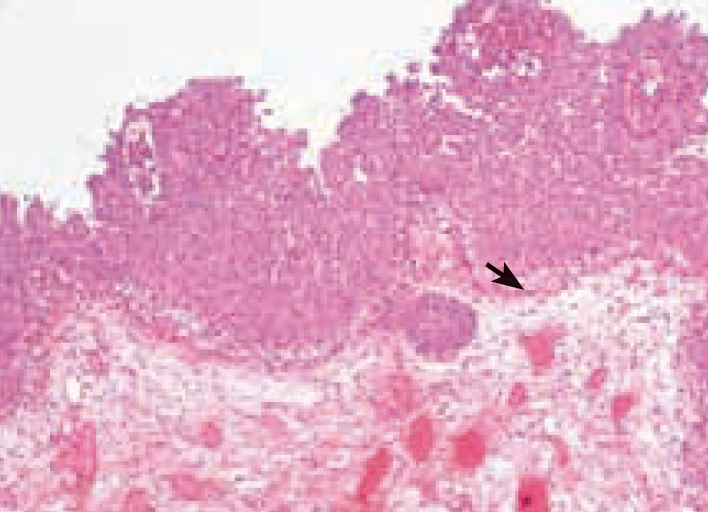
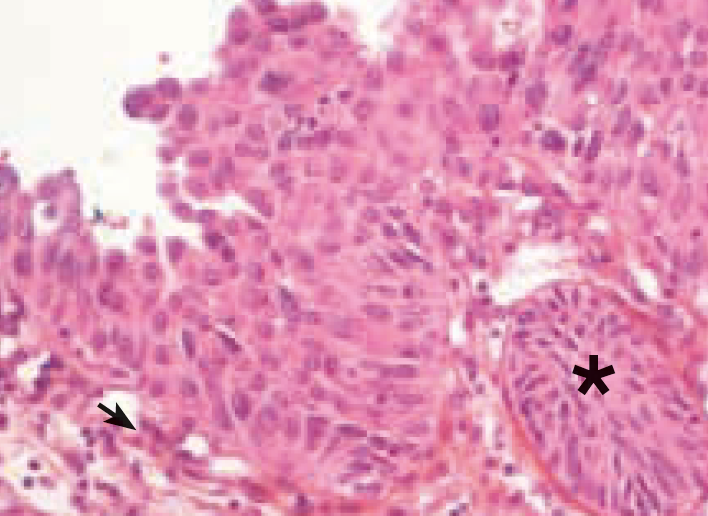
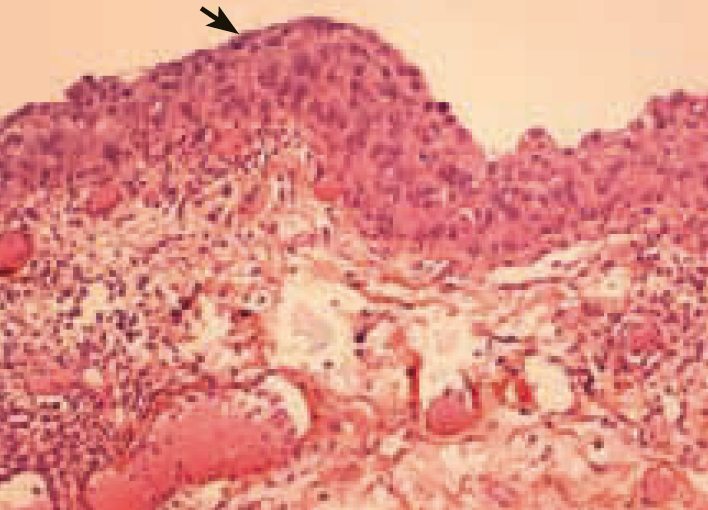
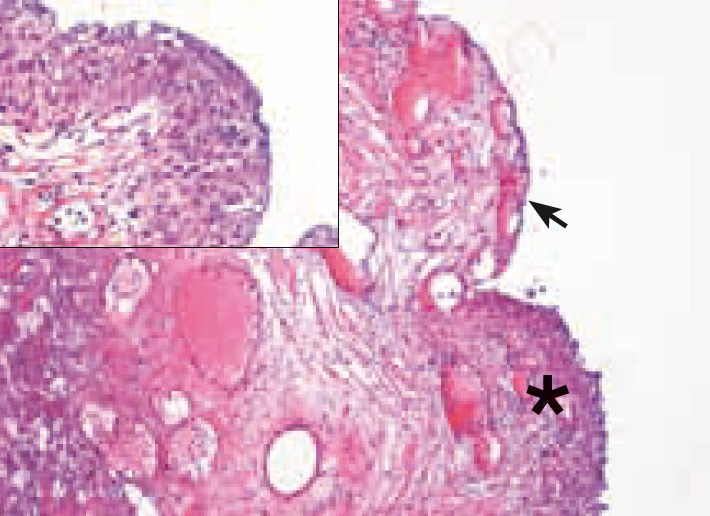
Low power is evocative of the erosive form of carcinoma in situ as the urothelial layer is detached (arrowhead) or denuded (*). At high power large pleomorphic cells with abundant cytoplasm are grouped in clusters and remain attached to the basal layer (arrowhead).
Case 6 CIS Male, aged 71

History
71 yo male, EBRT for prostate cancer seven years ago. Positive cytology with no evidence of disease on white light cystoscopy. Blue light shows a faint irregularity on the right bladder wall.

Pathology
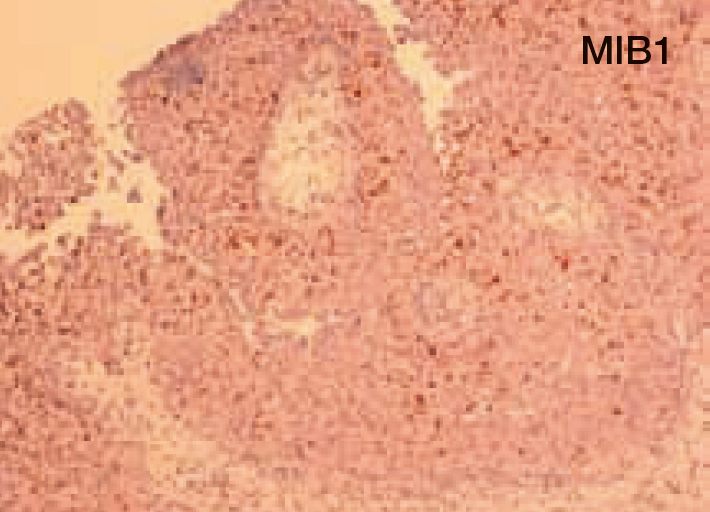
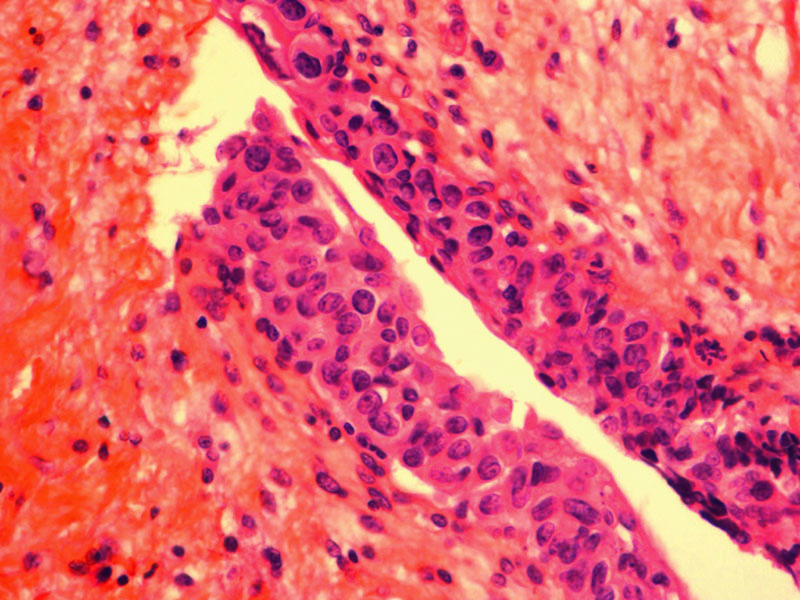
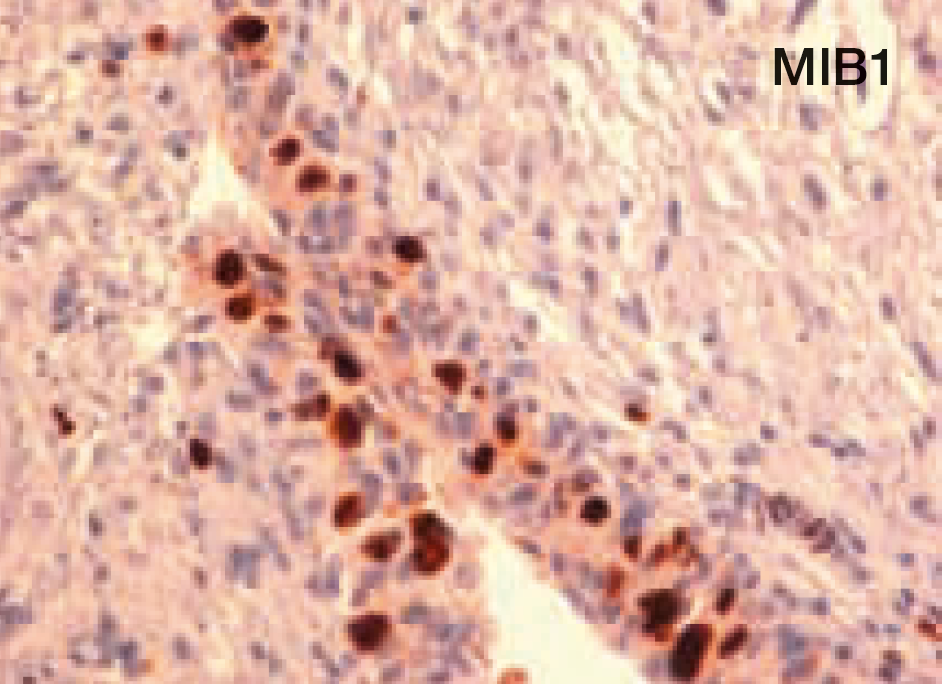
The urothelial layer is thin and disorganised. Note the presence of large proliferative cells with prominent nuclei (arrowhead). Proliferative cells (MIB1) are interspersed between normal cells in a pagetoid variant of carcinoma in situ.
Case 7 CIS Male, aged 70


History
70 yo male with history of pT1G3 treated by BCG + maintenance. Positive cytology but unevocative white light cystoscopy spurred two successive random biopsies that failed to show any significant abnormalities. Blue light showed three large flat and fluorescent areas whose detached urothelium was intensely fluorescent (inset).

Pathology
Low power shows denuded areas (arrowhead), when present (*) the urothelium appears normal. High power (box) shows faint abnormalities in the guise of slight architectural disorganisation and presence of large nuclei that were not sufficient to characterise carcinoma in situ. However, intense and discrete p53 staining confirms malignancy.
- Content Type