Case : Right lung tumor

Fumihiro Asano, MD, PhD
Department of Pulmonary Medicine,
Gifu Prefectural General Medical Center
Scope: BF-1TH1200
Case:Right lung tumor
Location:From the lower trachea to the right main bronchus
Patient information: Male, 70 years old
Medical history:Having experienced a persistent cough for about 1 month, the patient went to a local clinic. A chest X-ray revealed an abnormal shadow in the right middle lung field, and he was referred to our institution.
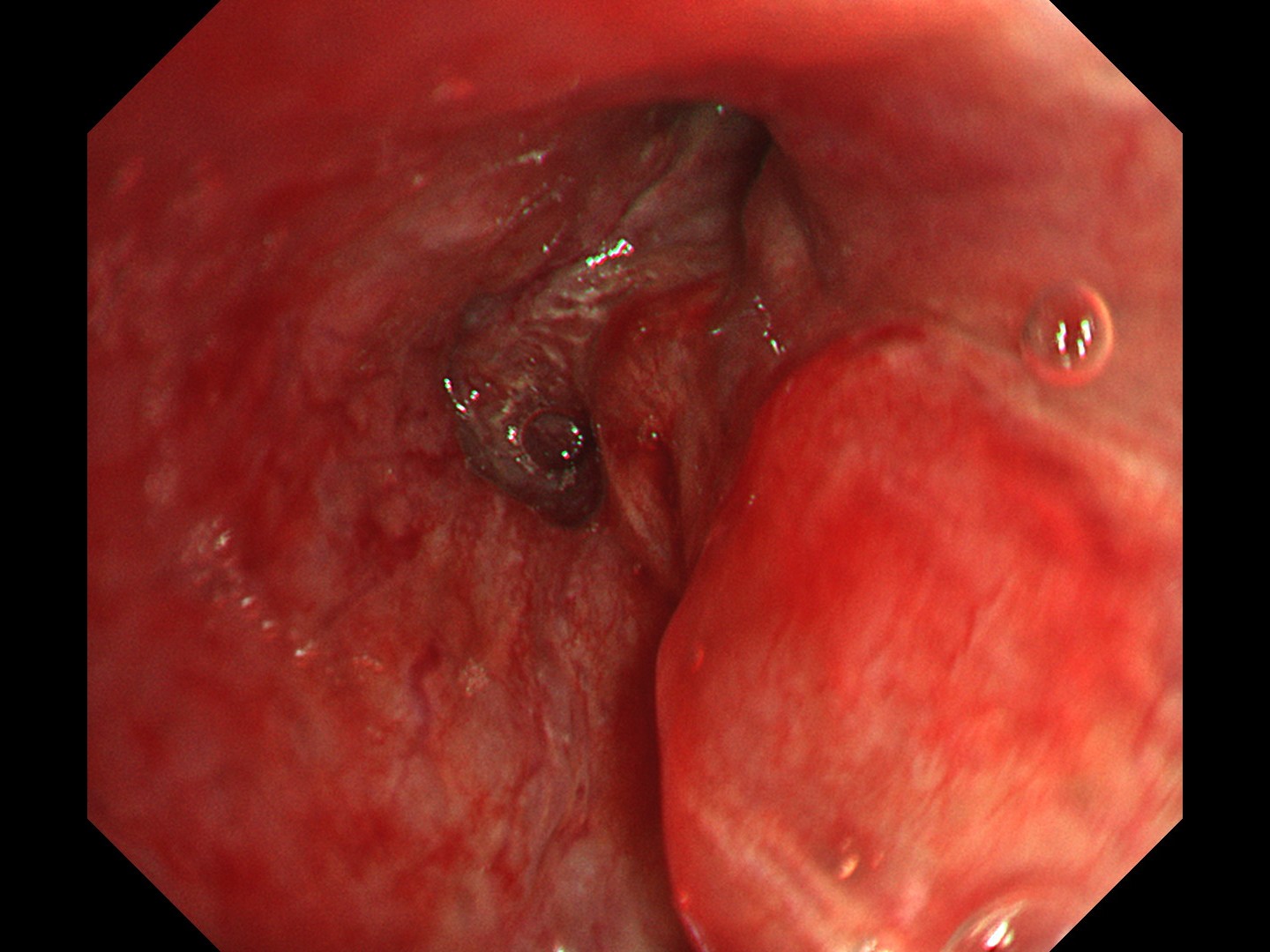
1-1 Tracheal bifurcation (WLI)
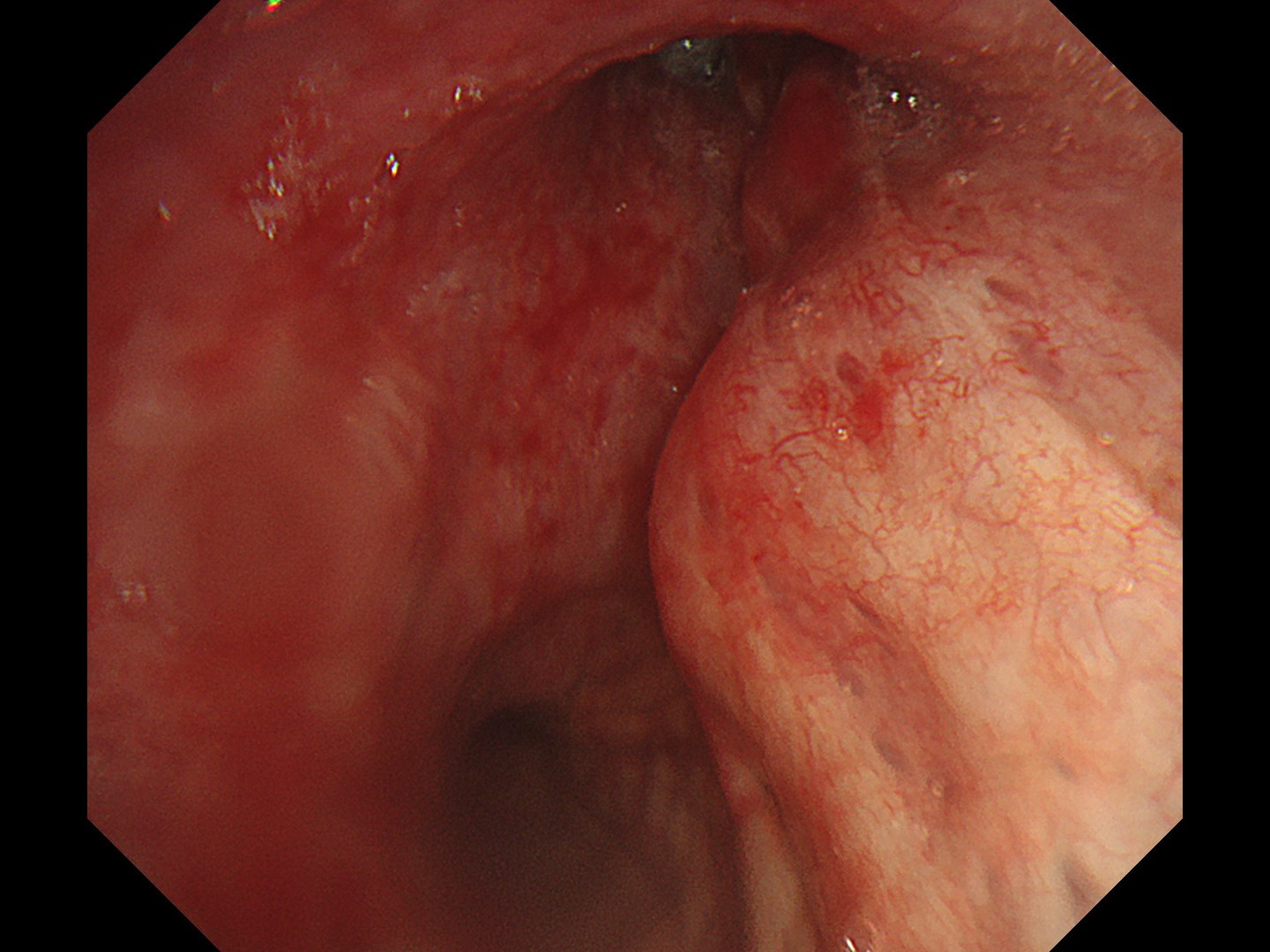
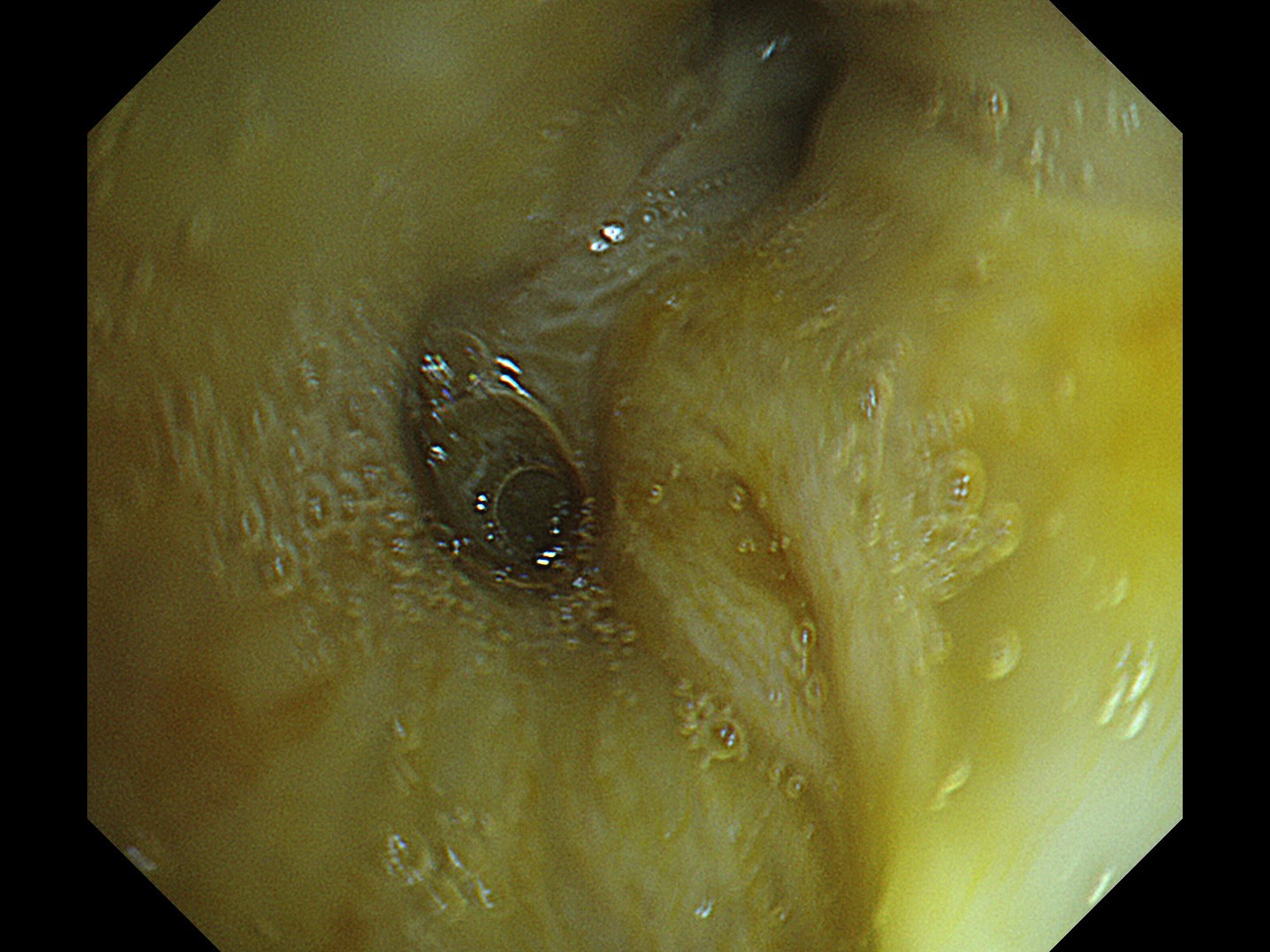
1-2 Tracheal bifurcation (TXI)
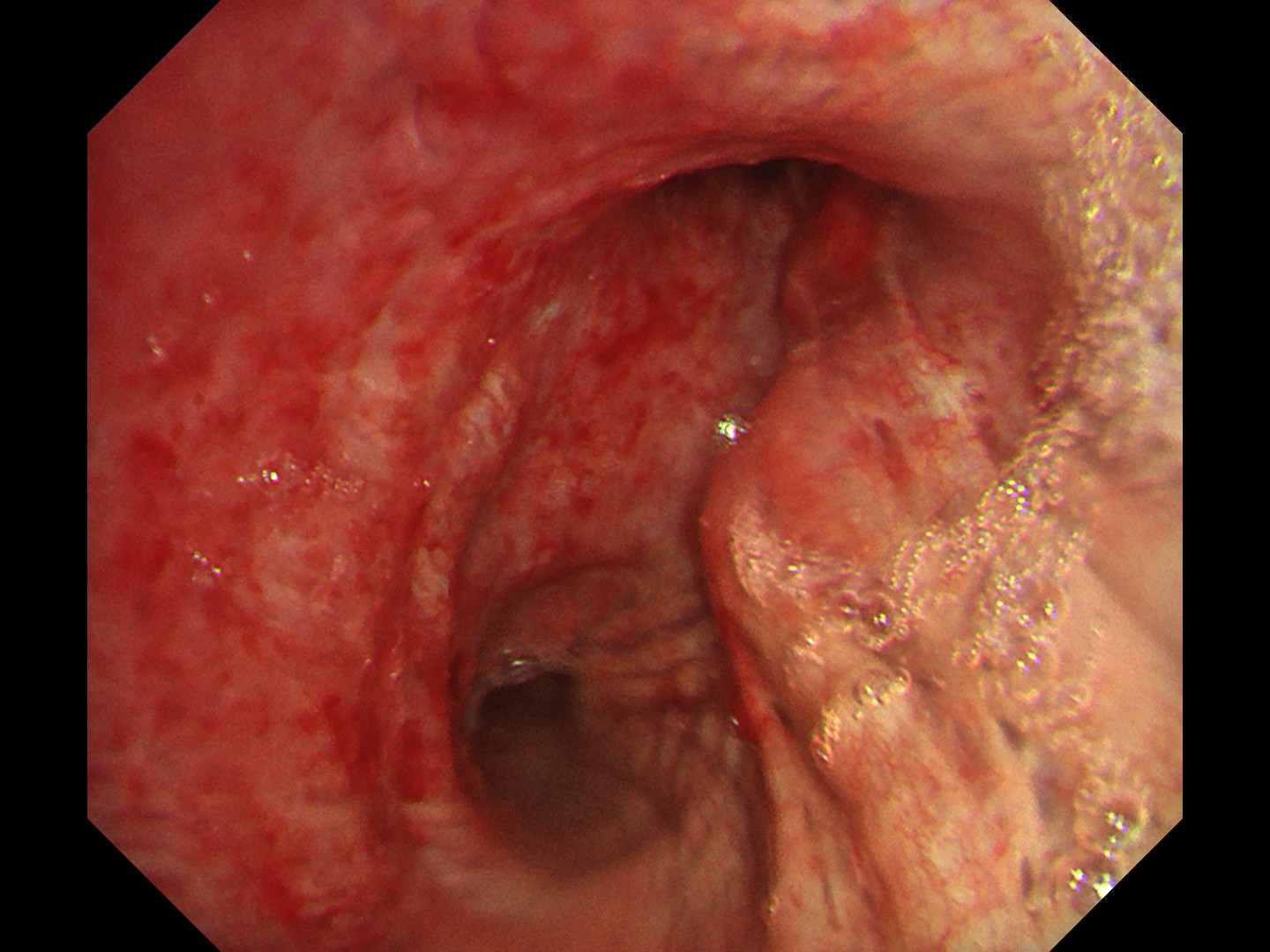
1-3 Right main bronchus (WLI)
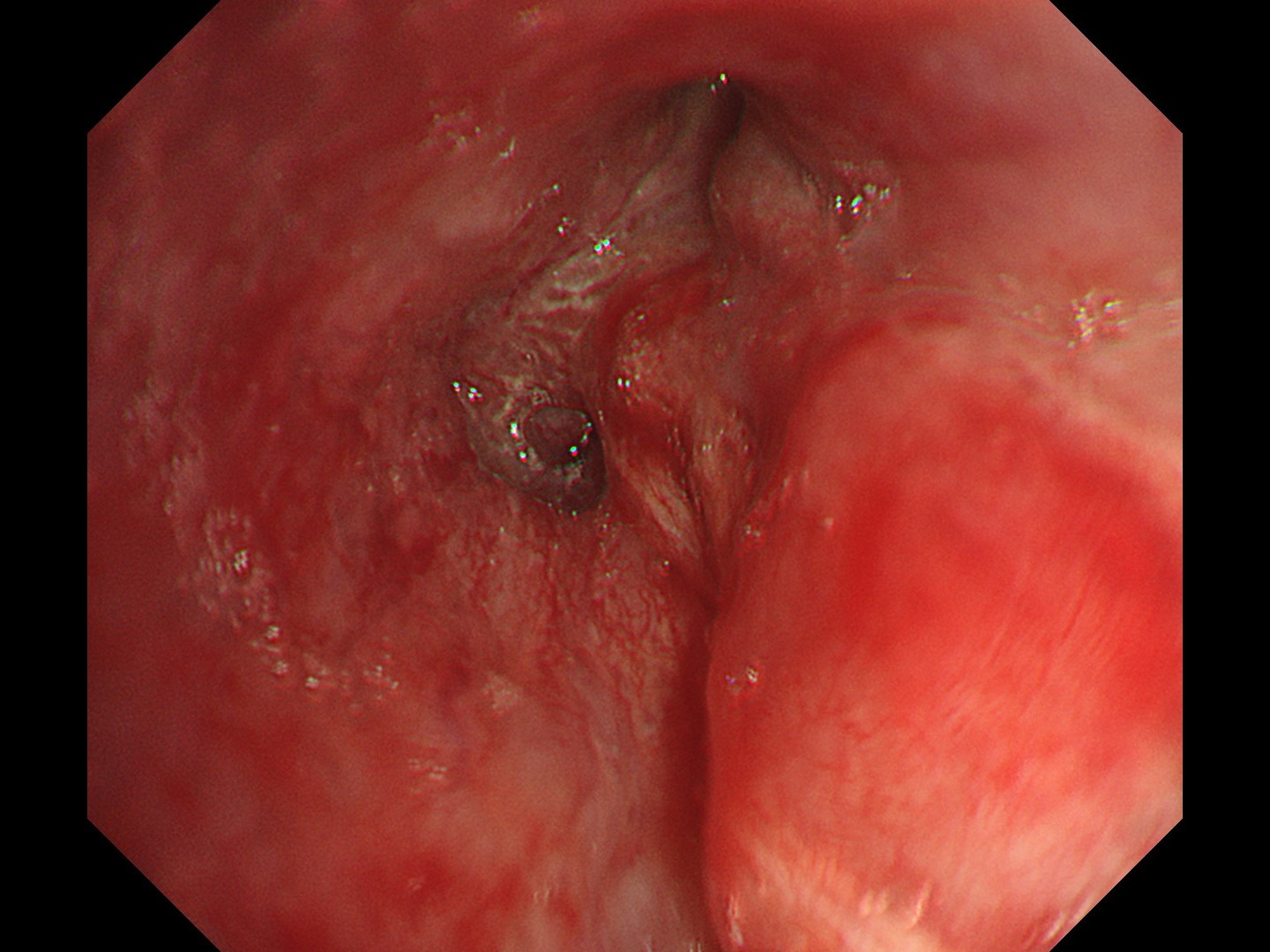
1-4 Right main bronchus (TXI)
1-5 Right main bronchus (RDI)
Pathological Findings
Endoscopic biopsy and EBUS-TBNA of mediastinal lymph node revealed:
- Small cell carcinoma (poorly differentiated neuroendocrine carcinoma)
- Diffuse proliferation of atypical cells with high N/C ratio and small, round, naked nuclei; synaptophysin (+), chromogranin A (+), CD56 (+), TTF-1 (+), and LCA (-)
Overall Comment
This was a case of small cell carcinoma originating from the right upper lobe (c-T4N3M1, stage IV), with bronchoscopy findings showing widespread progression of the small cell carcinoma from the subepithelial layer to inside and outside the bronchial wall. TXI mode enhances the visualization of SCLC that has spread widely beyond the bronchial wall, compared to white light. Additionally, it allows for clear observation of distal areas without causing halation in proximal areas, enabling easier determination of the extent of invasion.
- Content Type