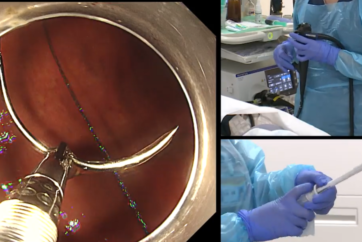
Image of Continuous Suturing (When the GIF-H290T Is Used)
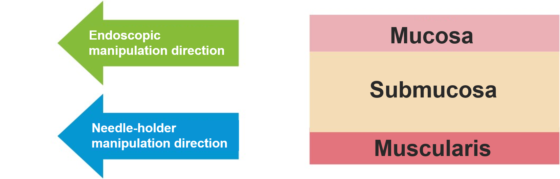
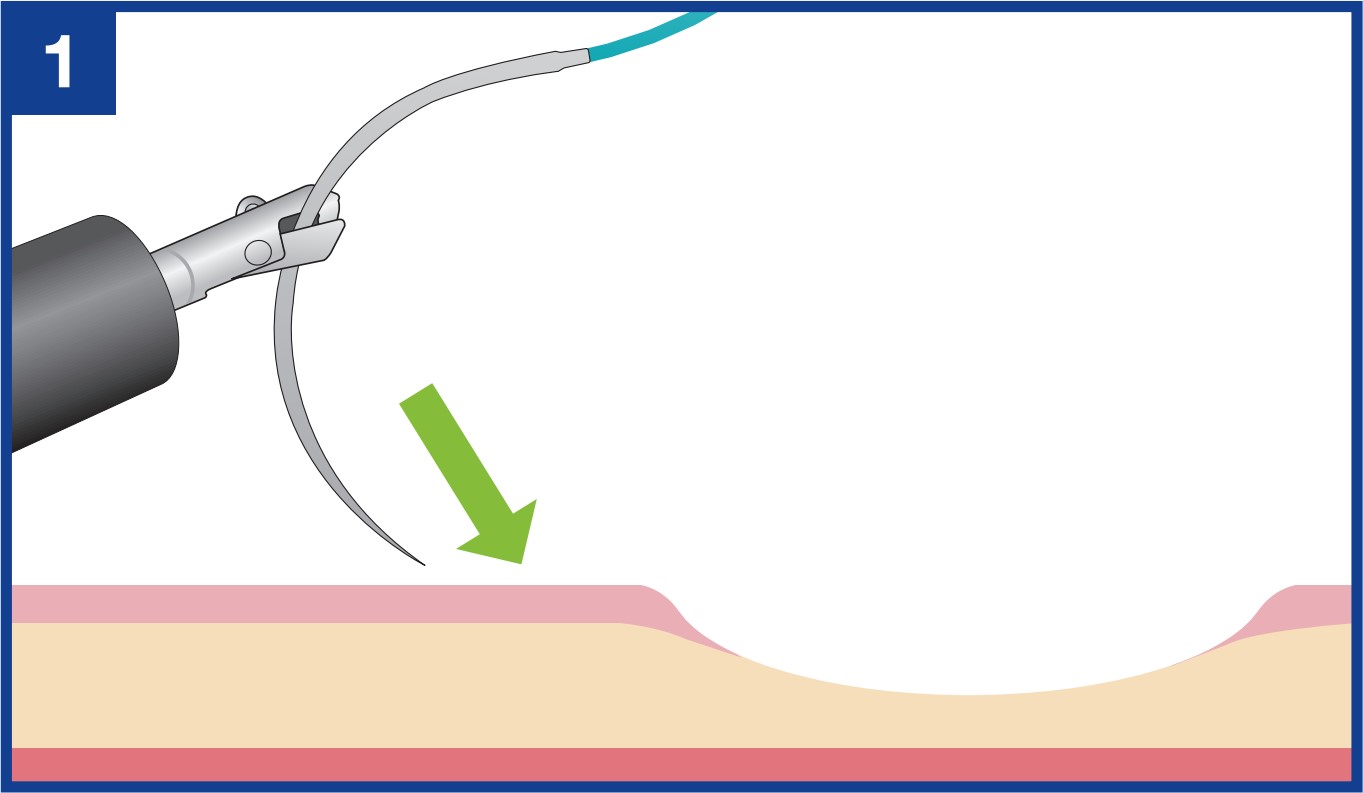
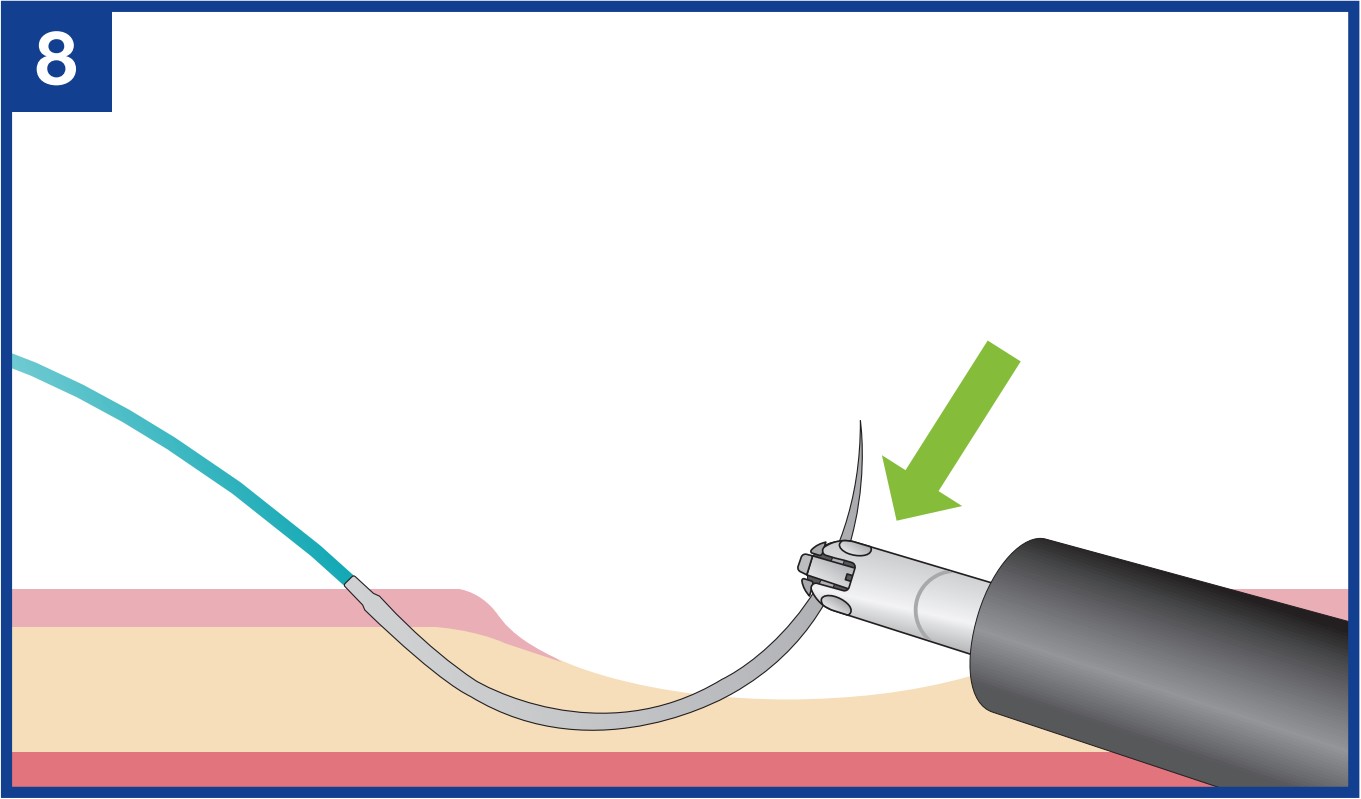
The endoscopist pierces the needle obliquely and stops at the desired depth. This trick helps you control the depth of suturing. Be careful not to pierce the needle too deeply.
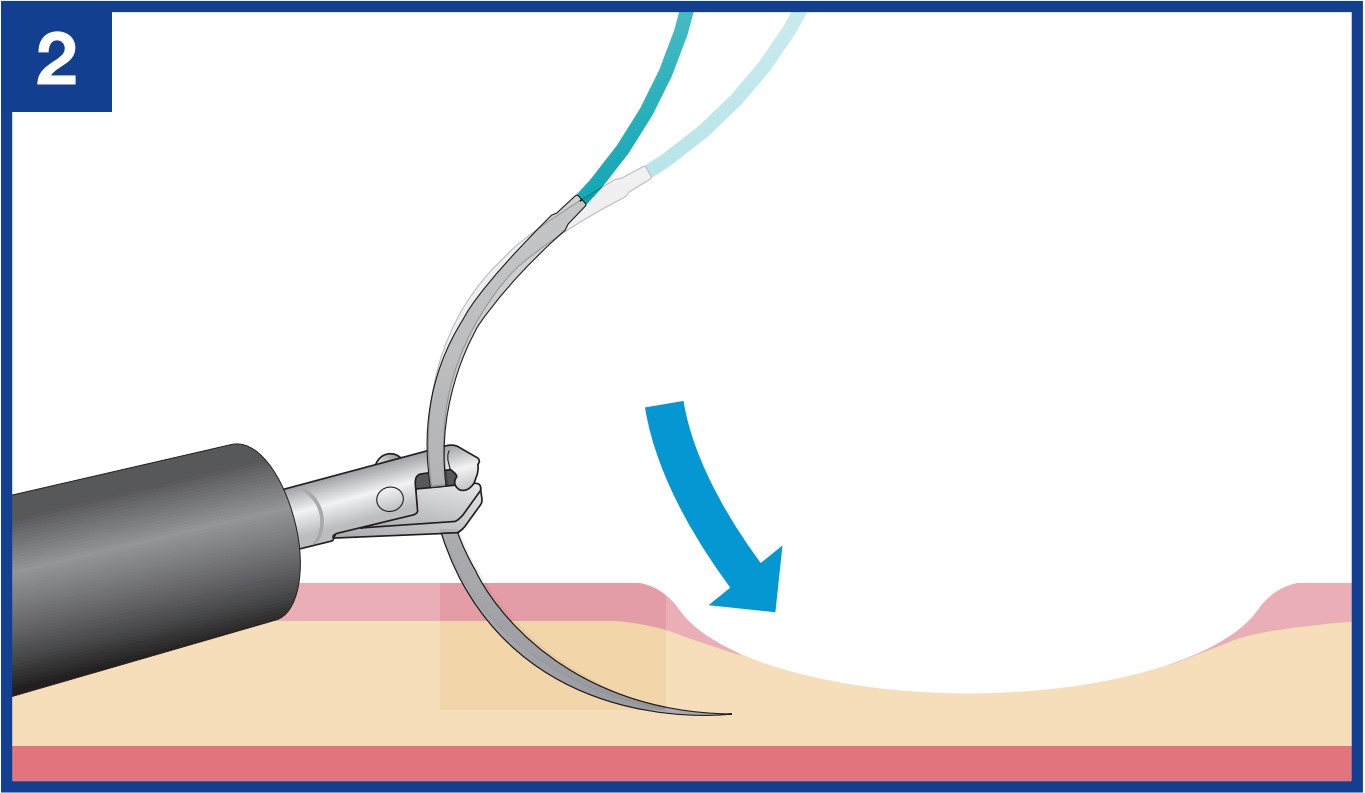
The assistant twists the needle-holder until the needle point is pointing parallel to the tissue surface. This helps control suture depth.
The endoscopist advances the needle in parallel to the tissue surface. This ensures a suture “bite” (the distance from the point of insertion of the needle to the edge of the mucosal defect) .
If there is no choice other than piercing downward, controlling the penetration depth is especially important. As soon as the endoscopist has punctured the surface of the tissue using endoscopic maneuvers, the assistant immediately twists the needle-holder to point the tip of the needle parallel to the tissue.
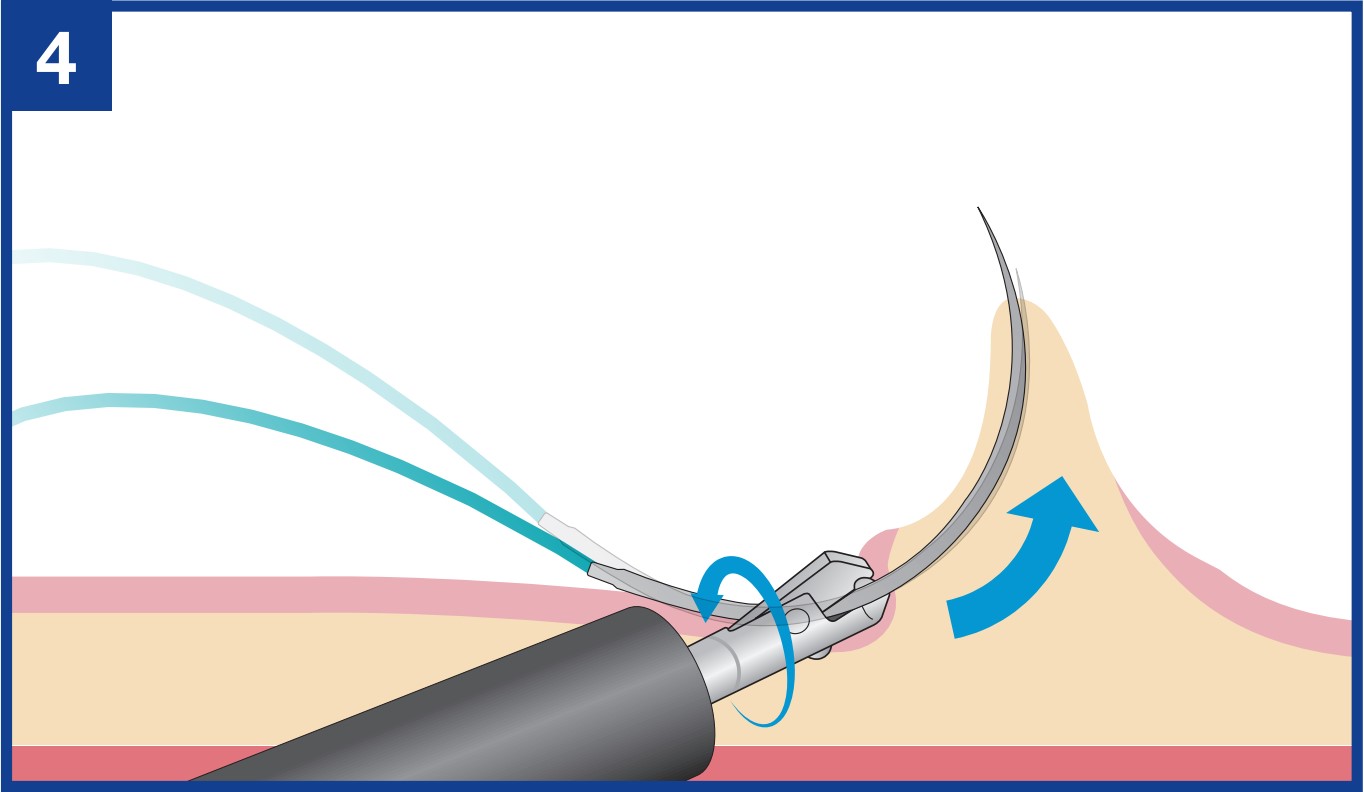
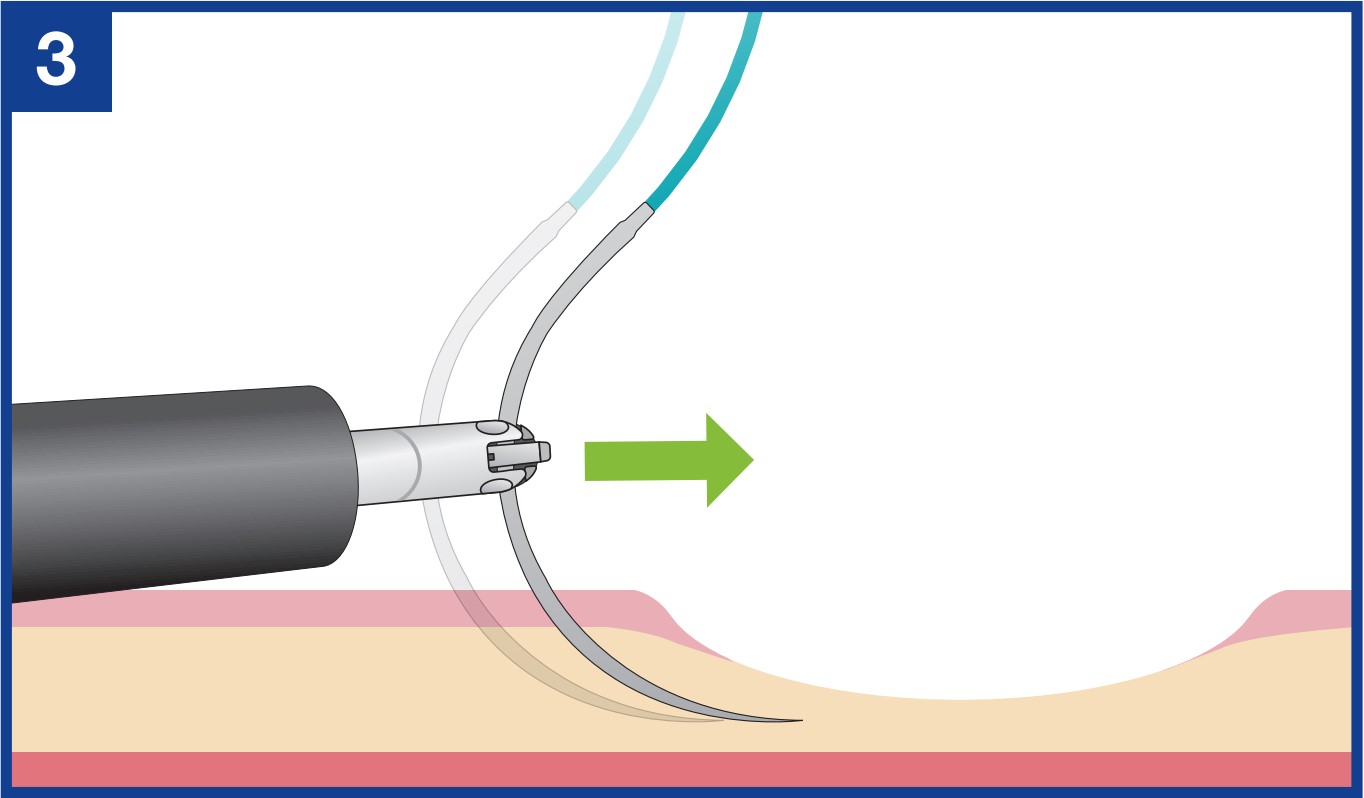
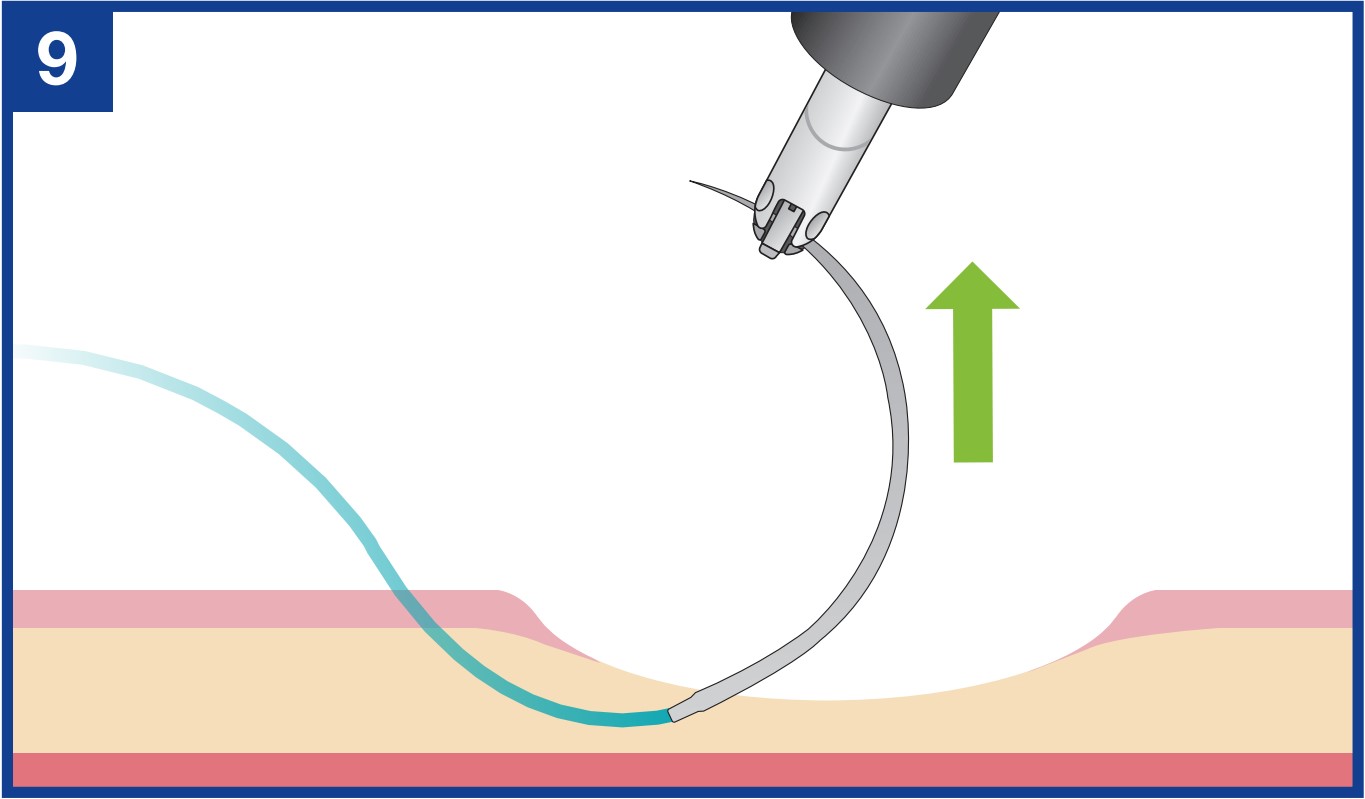
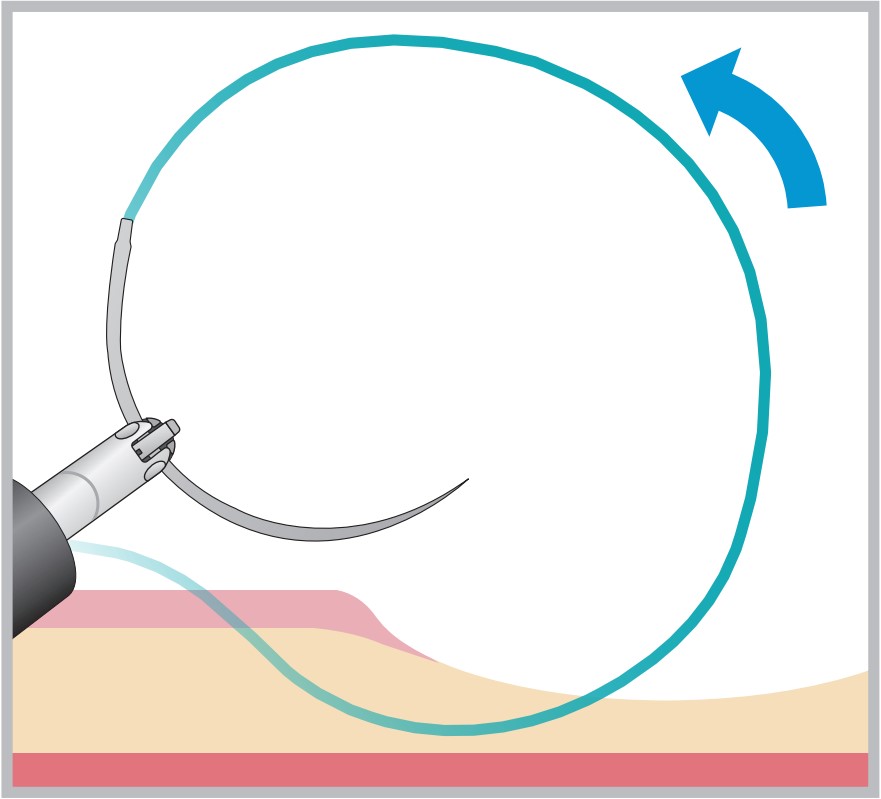
The assistant twists the needle-holder to apply force in the direction of the needle point to bring the needle point out of the tissue.
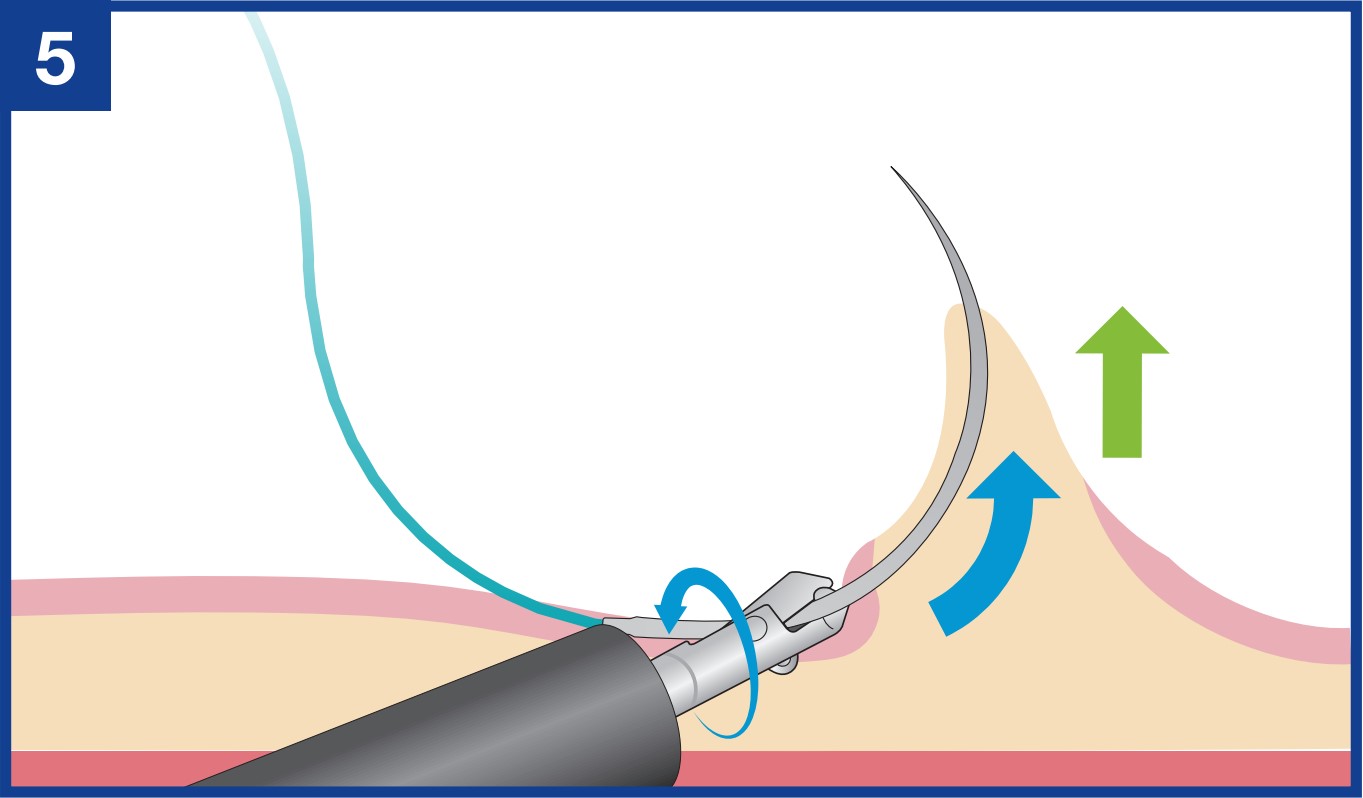
After twisting the needle-holder to project the needle point as necessary, the assistant then twists the needle-holder back towards the original position until no tension is applied to the tissue.
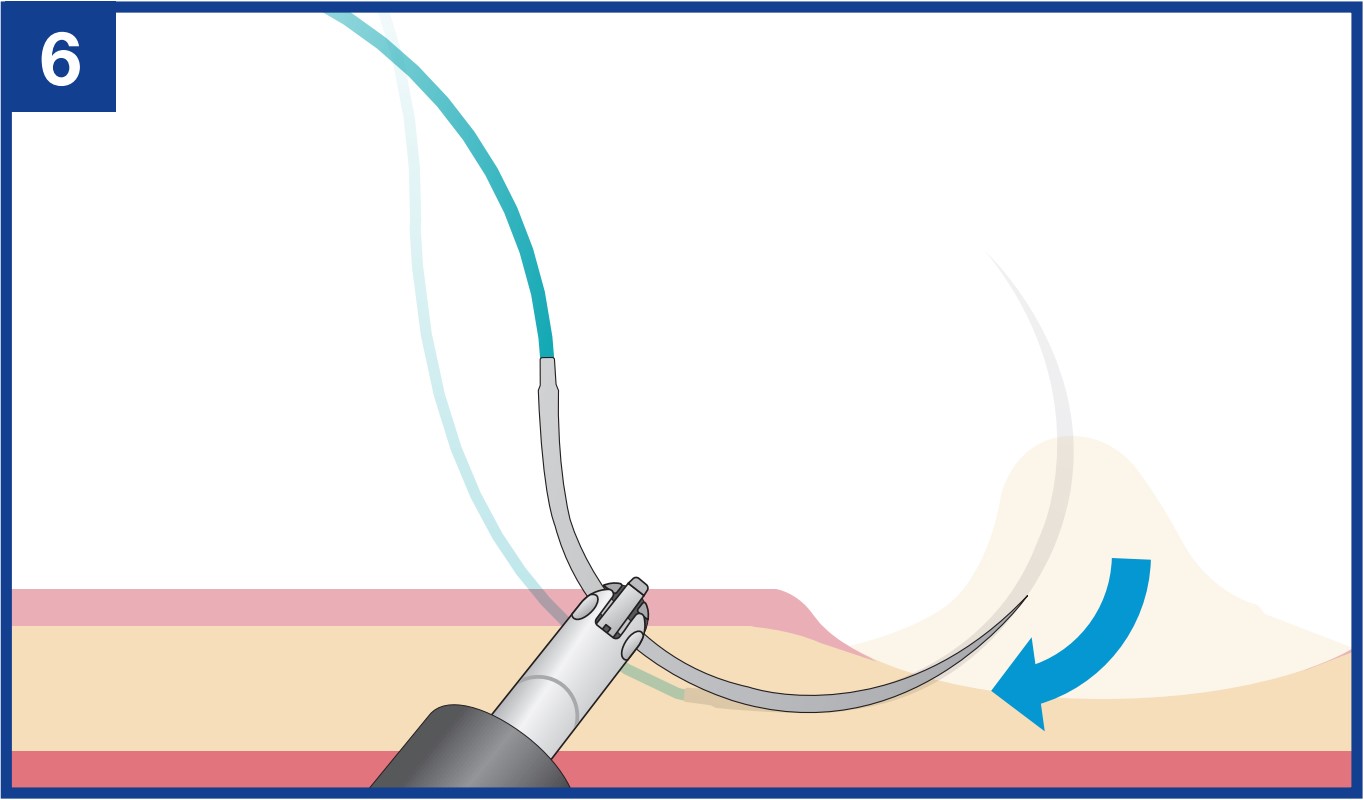
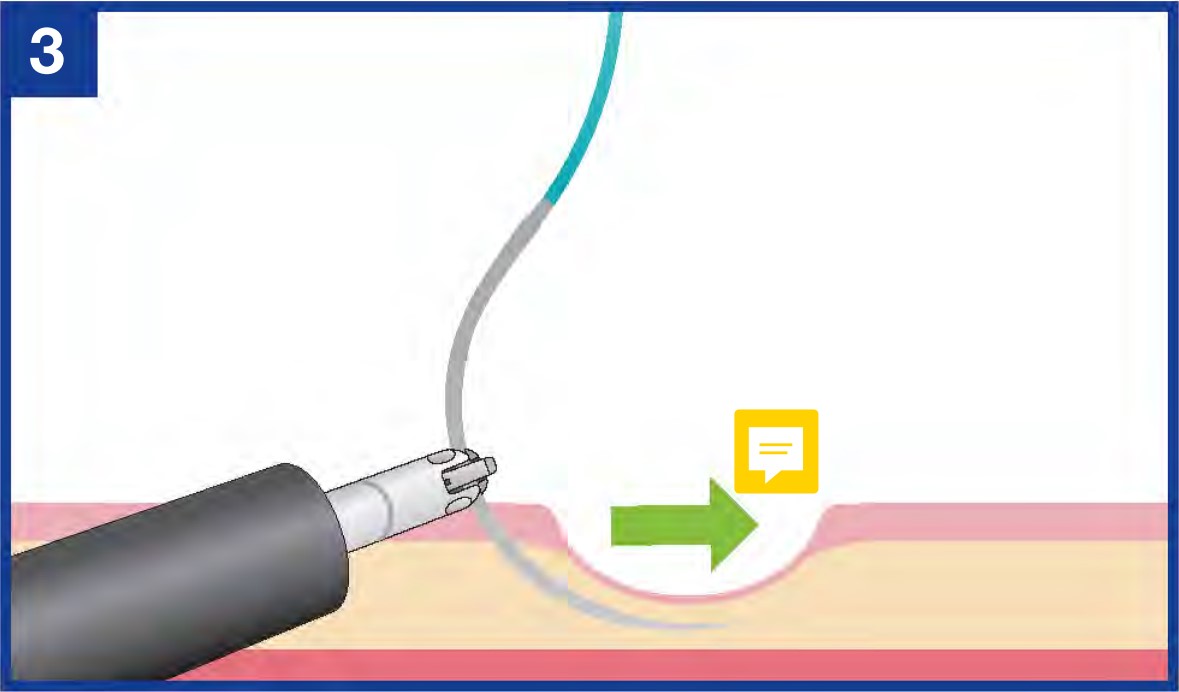
Once the needle is sufficiently penetrated through the mucosa, return the needle-holder to its original rotation until no tension is applied to the tissue. This helps prevent the needle point from getting stuck in the tissue due to the reaction caused by the application of tension to the mucosa when the needle is released.
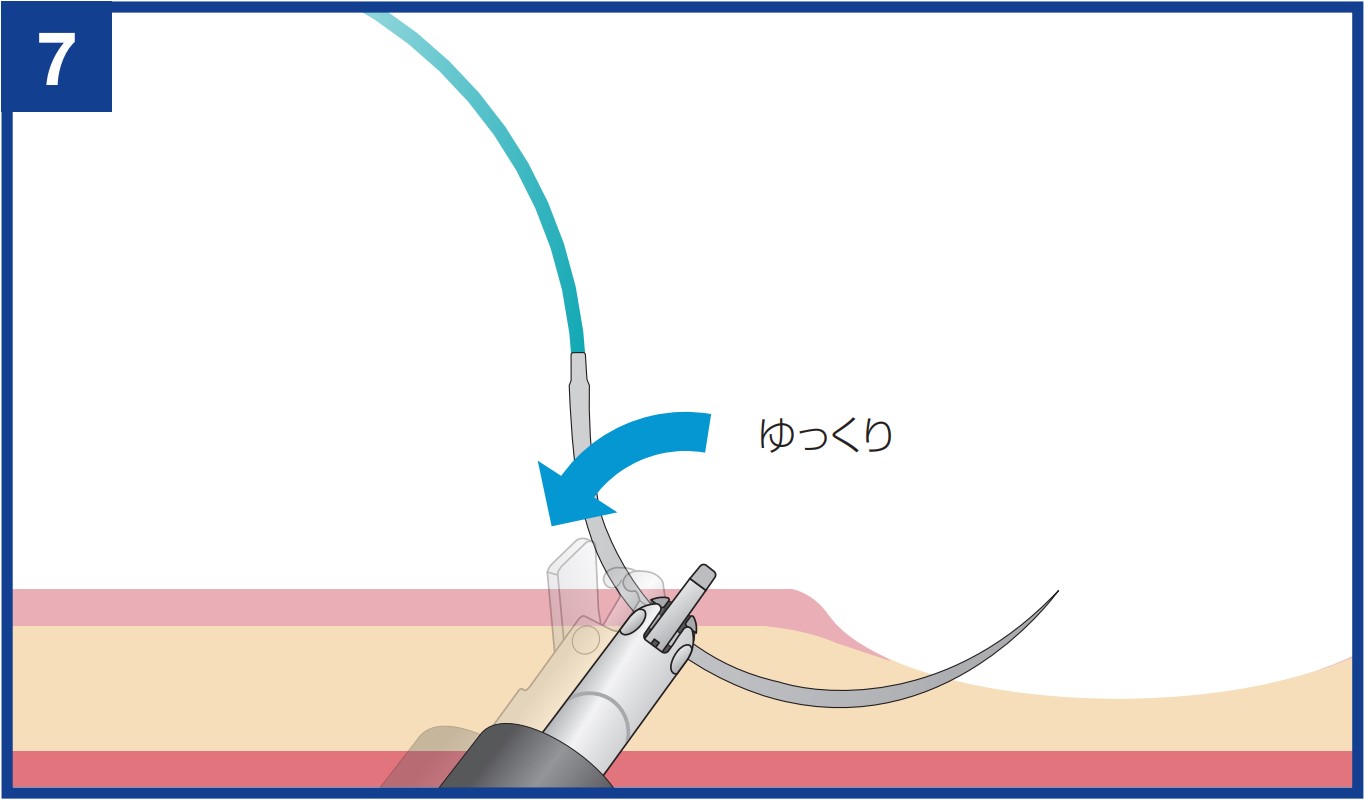
The assistant slowly opens the jaw on the tip of the needle-holder and, while the jaw is kept fully open, twists the needle-holder counterclockwise to release the needle. This allows the needle to be released from the needle-holder smoothly.
The endoscopist manipulates the scope to help the assistant grasp the tip of the needle protruding from the mucosa.
The endoscopist pulls the needle upward using endoscopic maneuvers, stopping while part of the needle is still in the tissue. (This is easier to do using only endoscopic maneuvers without twisting the needle-holder.) This facilitates regrasping of the needle.
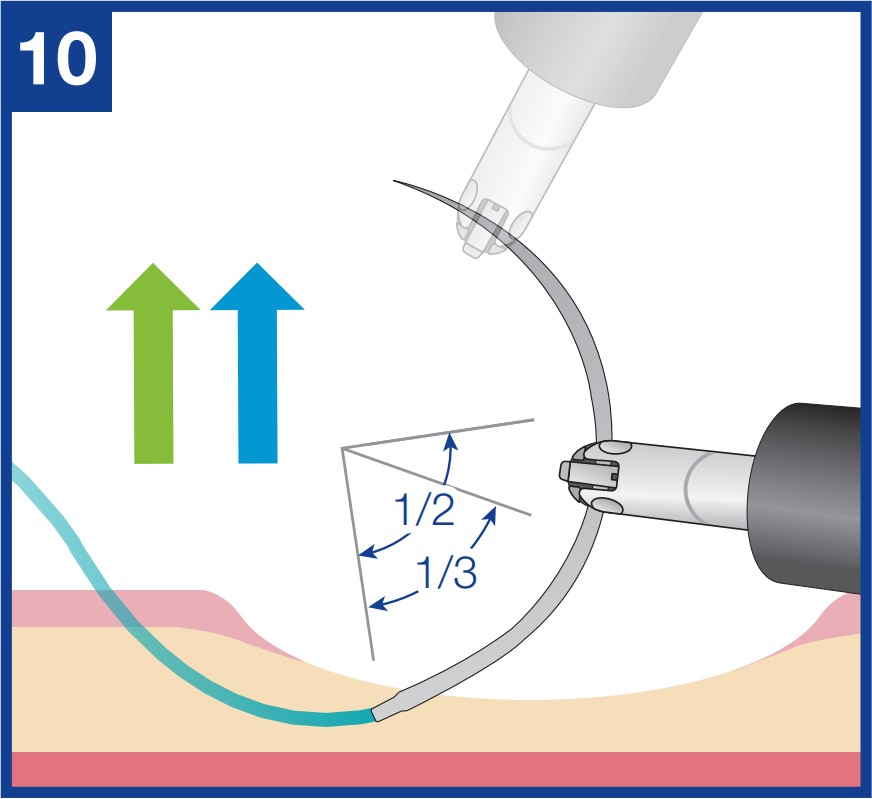
Release the needle once and regrasp the needle at a point 1/3–1/2 from the swaged end.
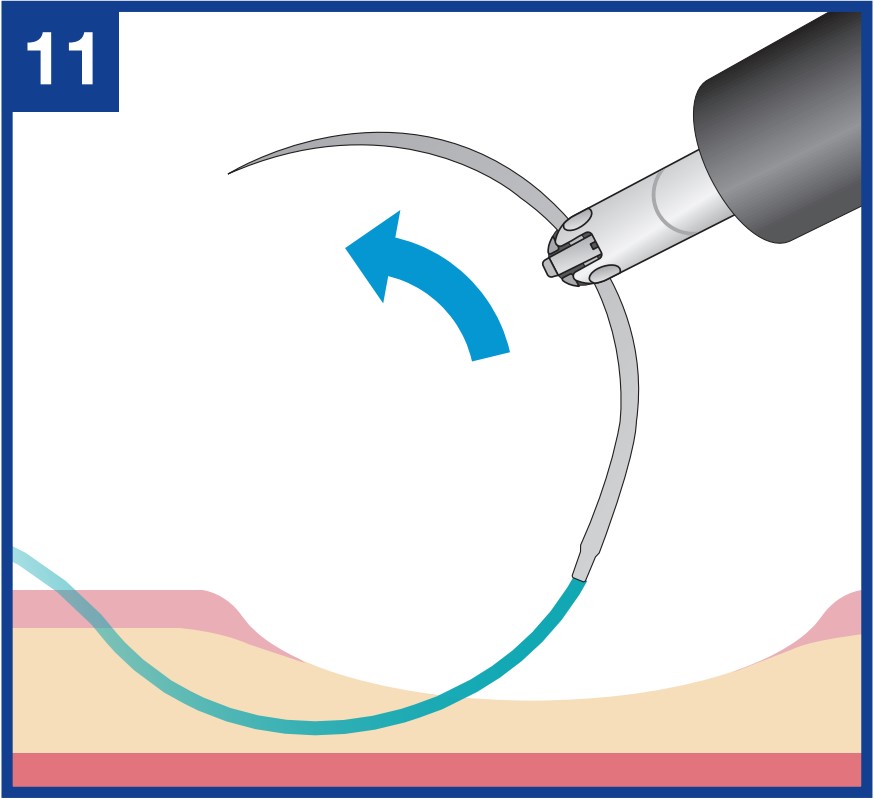
Pull out the needle completely. Then twist the needle-holder counterclockwise to move on to the next puncture. This keeps the suture from getting tangled.
- Content Type