CASE STUDY 5
Author
Doctor: Rosario Festa
U.O. Endoscopia Digestiva
IRCCS CROB – Rionero in Vulture (PZ) – Italy
Patient History and Findings
Male patient, 45 years old, with distal esophageal cancer, underwent distal esophagectomy and esophagus-stomach anastomosis in September 2015, with regular postoperative course.
He came to our attention, on the recommendation of a thoracic surgeon, for worsening dysphagia associated with significant weight loss.
Dilation Procedure with EZDilate
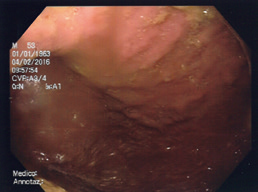
In January 2016, Esophagogastroduodenoscopy (EGD) was performed. At 28 cm from the dental archway, there was an anastomotic stenosis, not surmountable with a standard video gastroscope. Biopsies were performed in the anastomotic area and then the procedure was completed with a pediatric video gastroscope; there was no pathological evidence in the gastric mucosa, nor in the duodenum, explored until the second part.
Then, balloon dilation was performed up to Ø12 mm with HBD-W-10-11-12 by Cook Medical. Histology confirmed no mucosa alterations referable to any anastomotic recurrences.
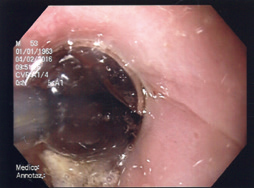
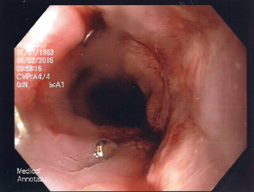
Three weeks later, the patient underwent a new endoscopic control to perform dilation with a 12 to 15 mm balloon. At the anastomosis site, the esophageal lumen appeared reduced in diameter, not surmountable with a standard video gastroscope, and surgical staples were clearly visible on the mucosa surface. Again, balloon dilation was performed with Cook HBD-W-12-13.5-15, but the balloon broke down at about 4atm.
After a few days, the patient was scheduled for a new EGD to perform balloon dilatation with Olympus EZDilate EGBD-410X-1555, which was inflated up to 4atm, Ø14.5 mm. This time, the stricture could be passed easily and the dilation was successful.
Outcome and Summary
The presence of the staples at the anastomosis level probably induced the HBD balloon to break. Therefore the different and more resistant material of the EZDilate balloon used in the last procedure may have permitted the effective completion of the pneumatic dilation of the esophagus stricture, despite the presence of the staples.

- Content Type