Disclaimer
The techniques and clinical opinions presented in this material reflect the personal experience and professional judgment of the healthcare professional and do not necessarily represent the views of Olympus. This material is intended for healthcare professionals only. Users should always refer to the applicable Instructions for Use (IFU) and use Olympus products in accordance with the approved indications and local regulatory requirements. The healthcare professional presenting this material has been engaged by Olympus and compensated at fair market value for their services.
Colorectal Case 36

Yasushi Sano 1.2
MD, PhD, FJGES, and ANBIIG 3
- Clinical Professor, Kansai Medical University Osaka, Japan
- Director & Chief of Gastrointestinal Center Sano Hospital, Kobe, Japan
- Secretary, Asian Novel Bio-Imaging and Intervention Group
Scope: CF-EZ1500DI
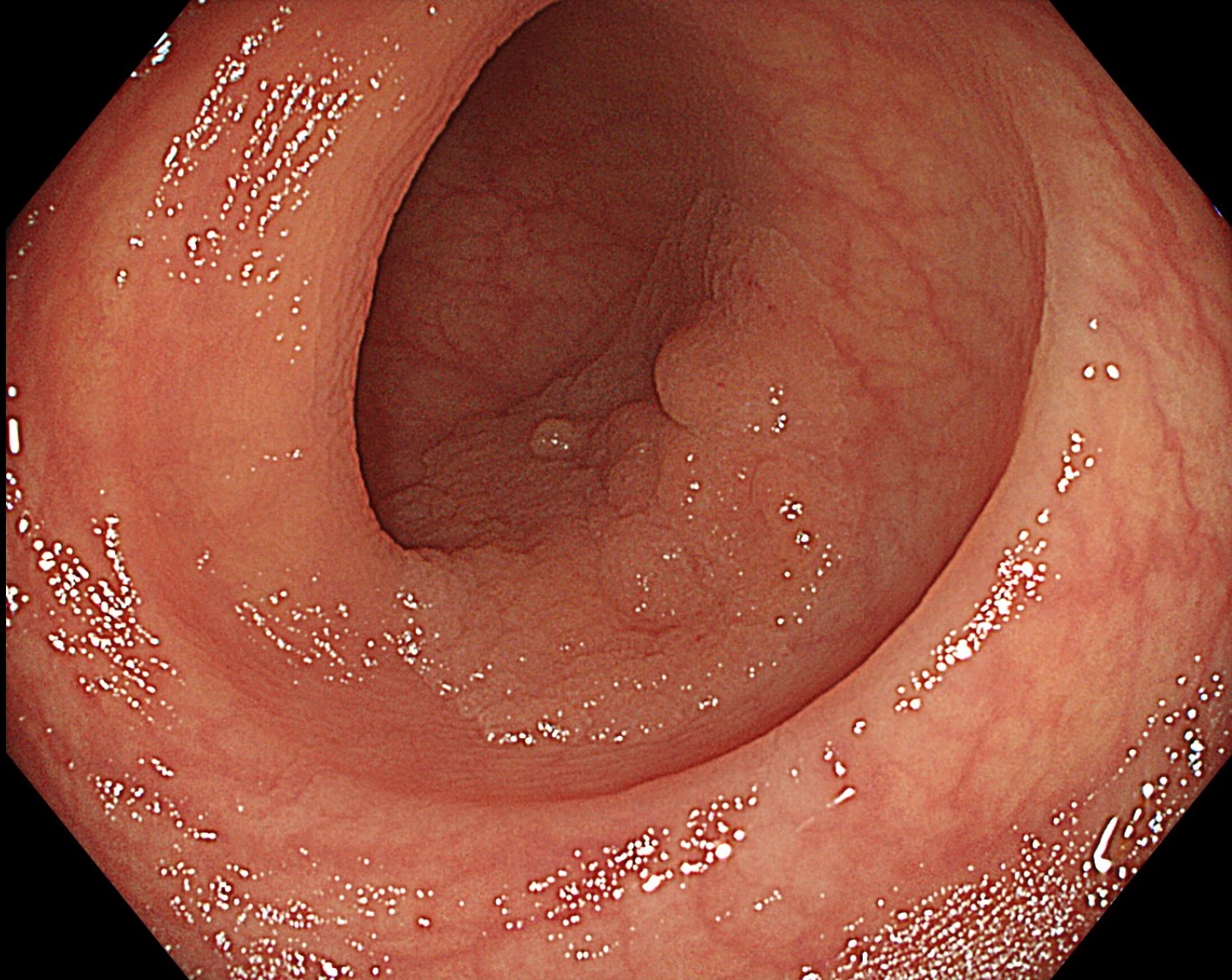
Case: Detection 0-IIa, SSL with CD
Site of lesion: Sigmoid colon
Patient information: F, 70s
Medical history: FOBT+
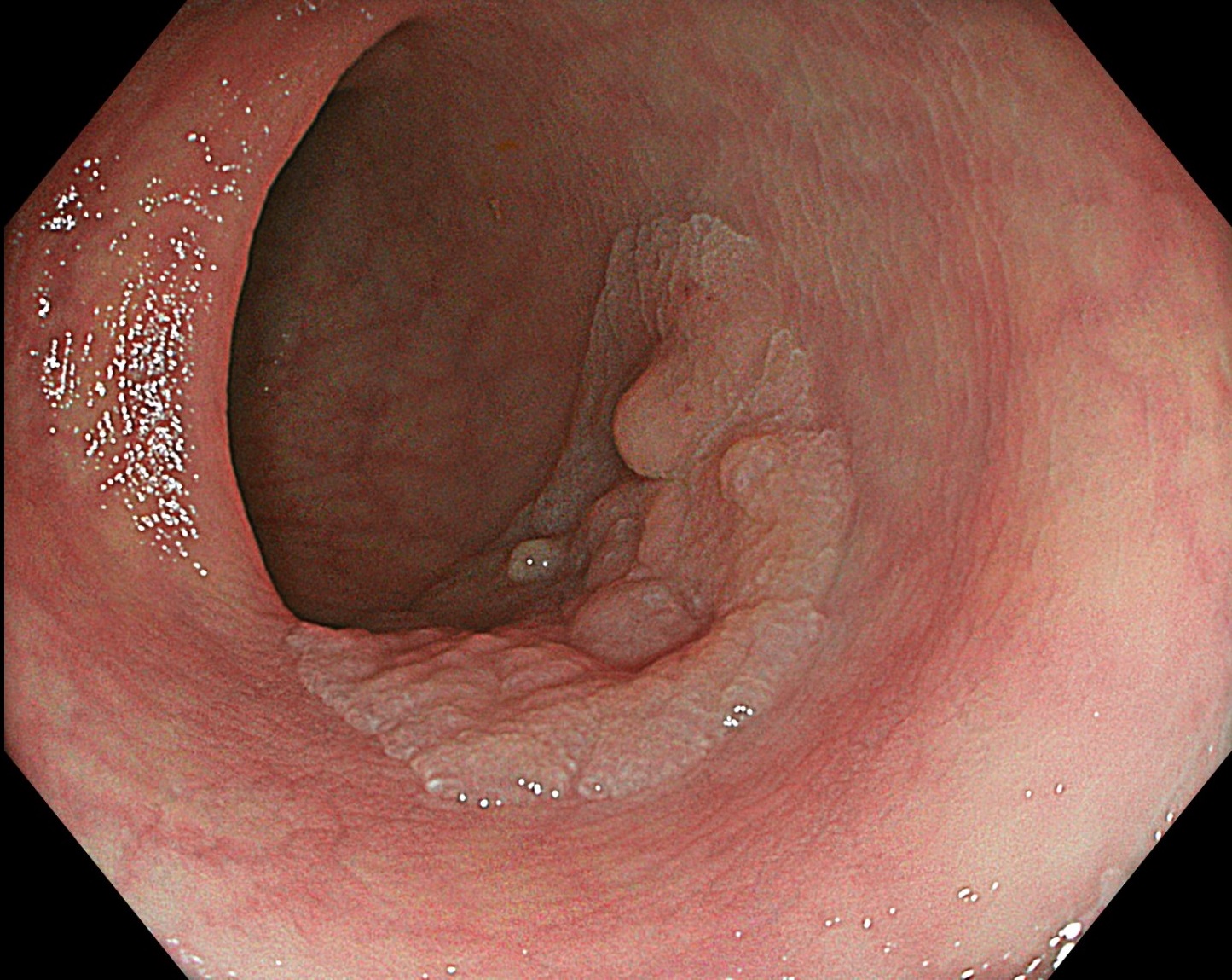
1. WLI
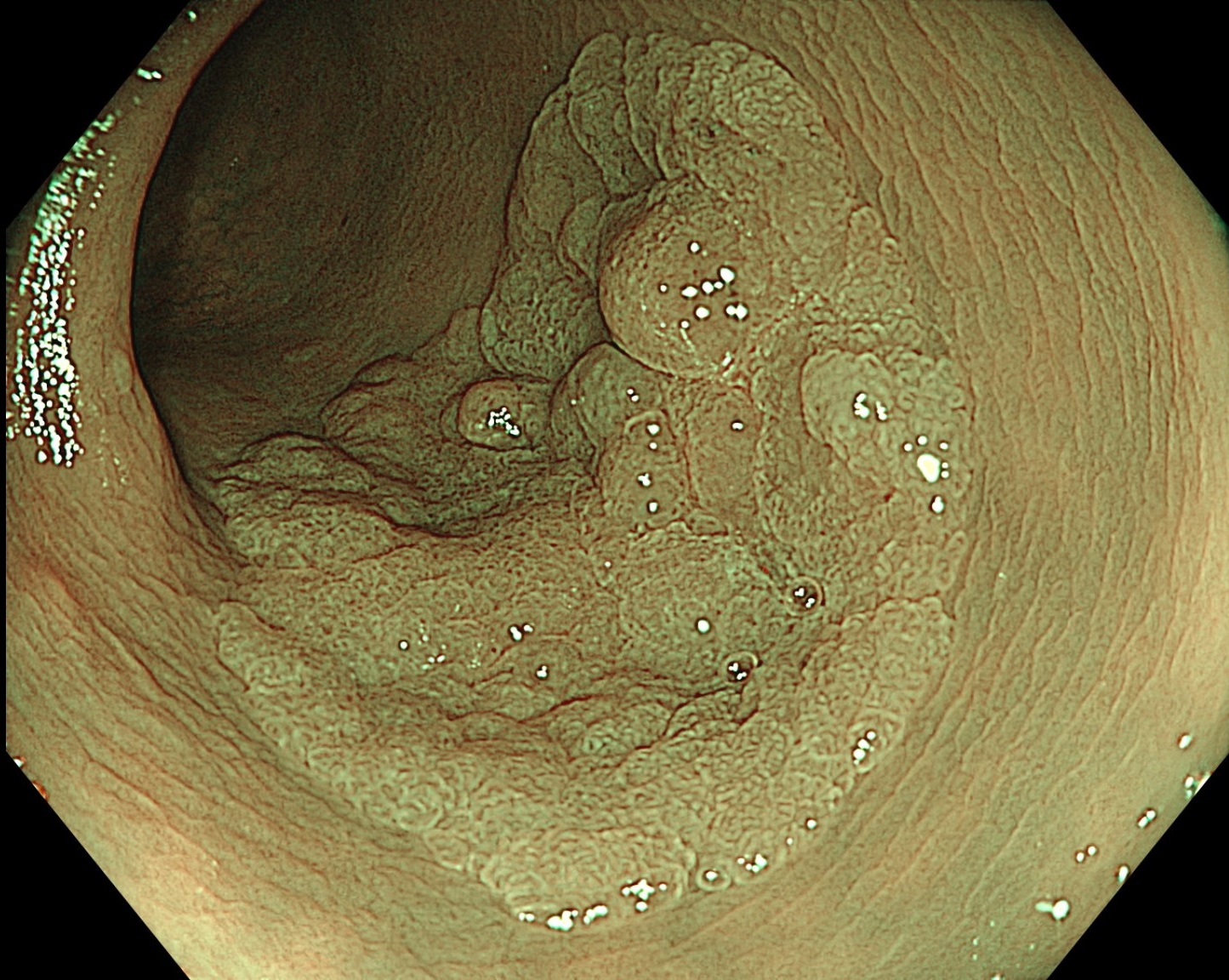
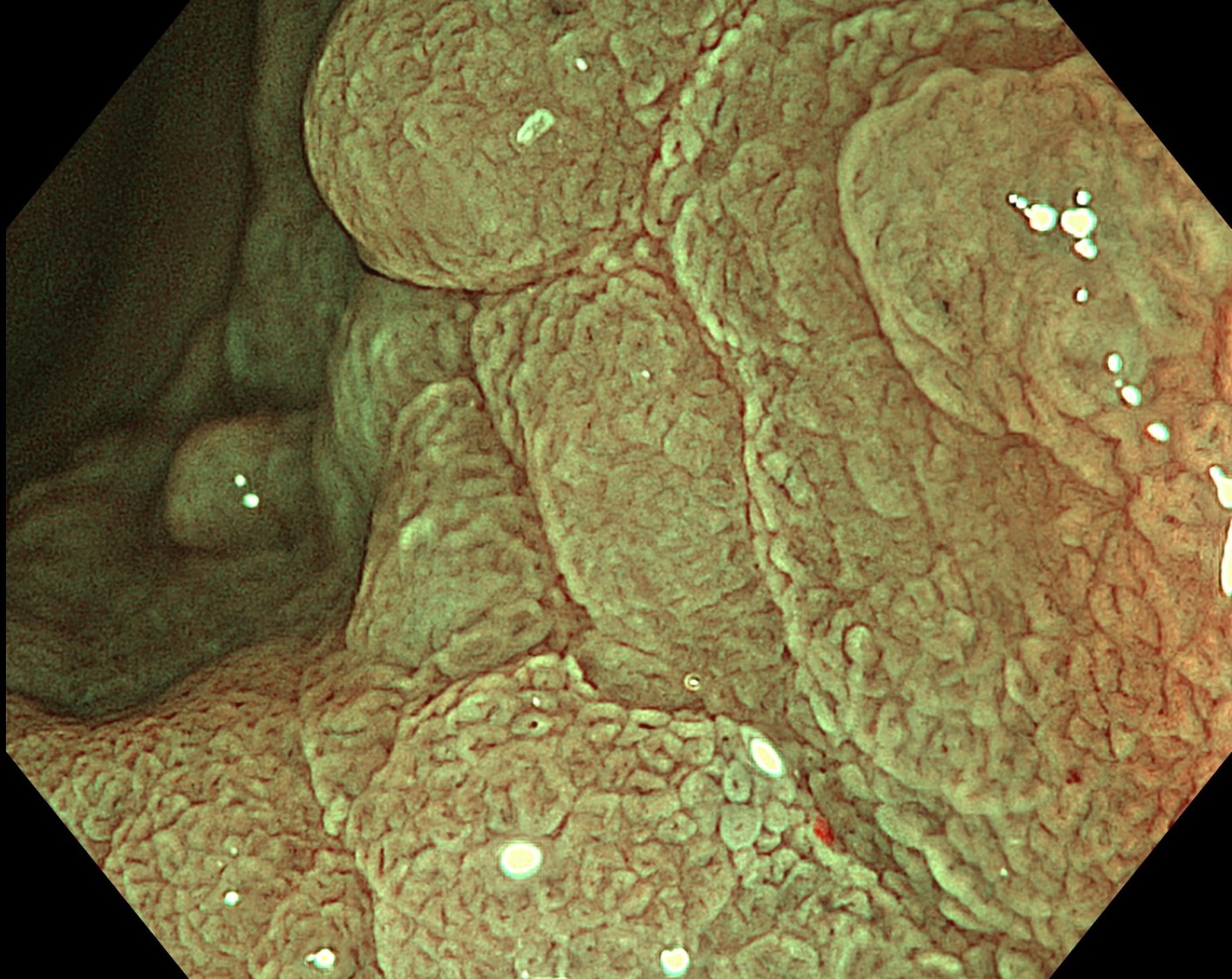
2. TXI
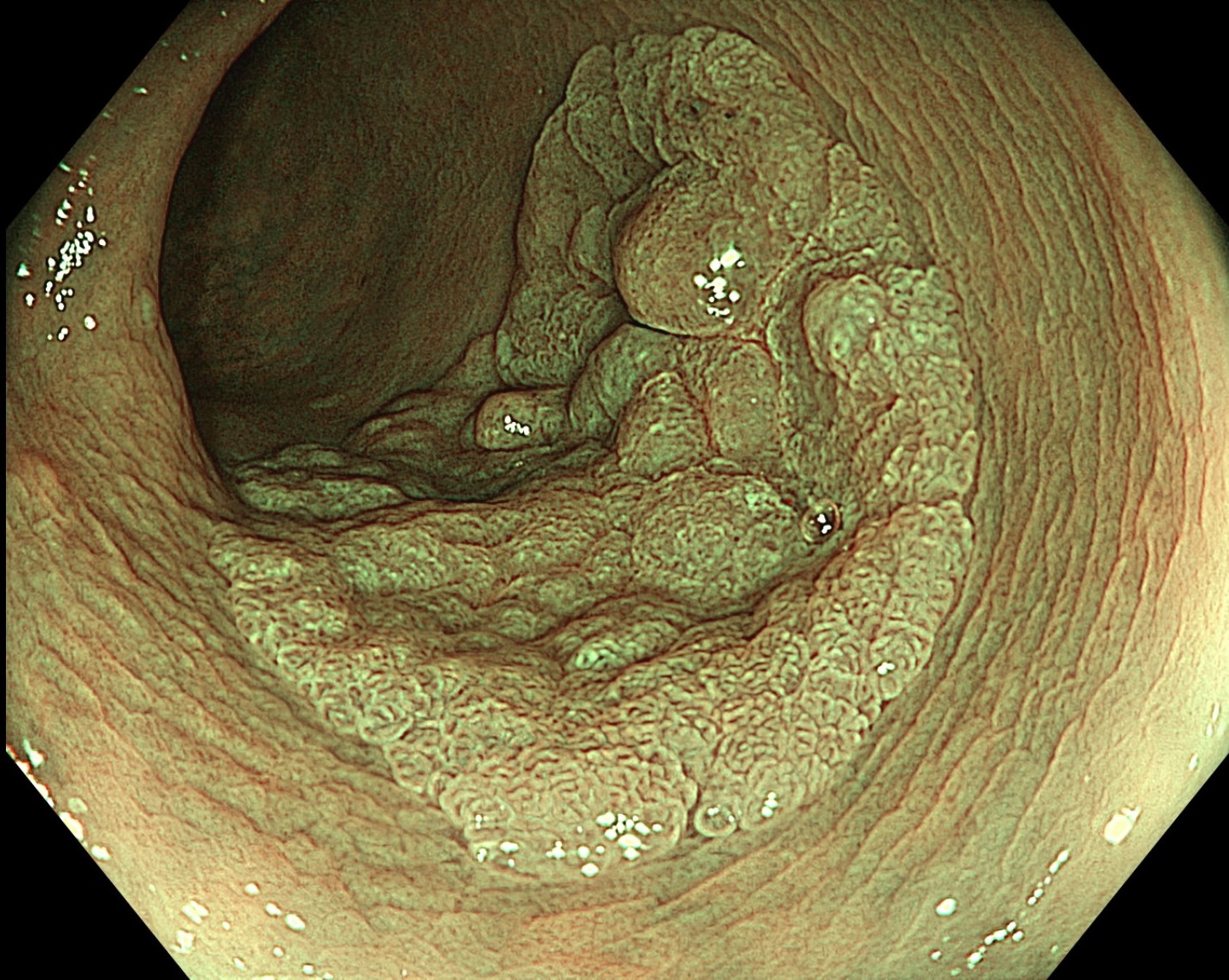
3. NBI
4. NBI+TXI
5. NBI+TXI
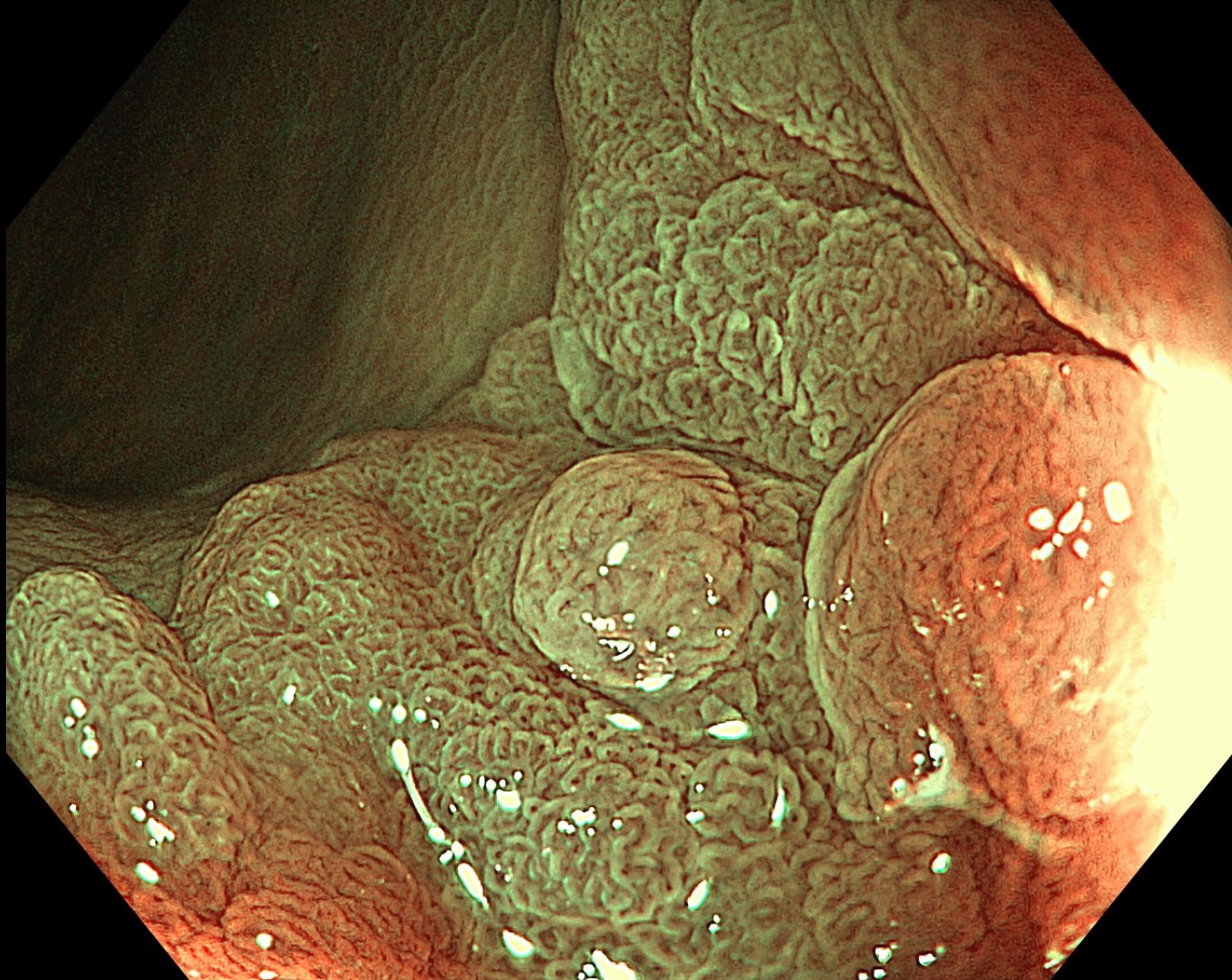
6. NBI+TXI
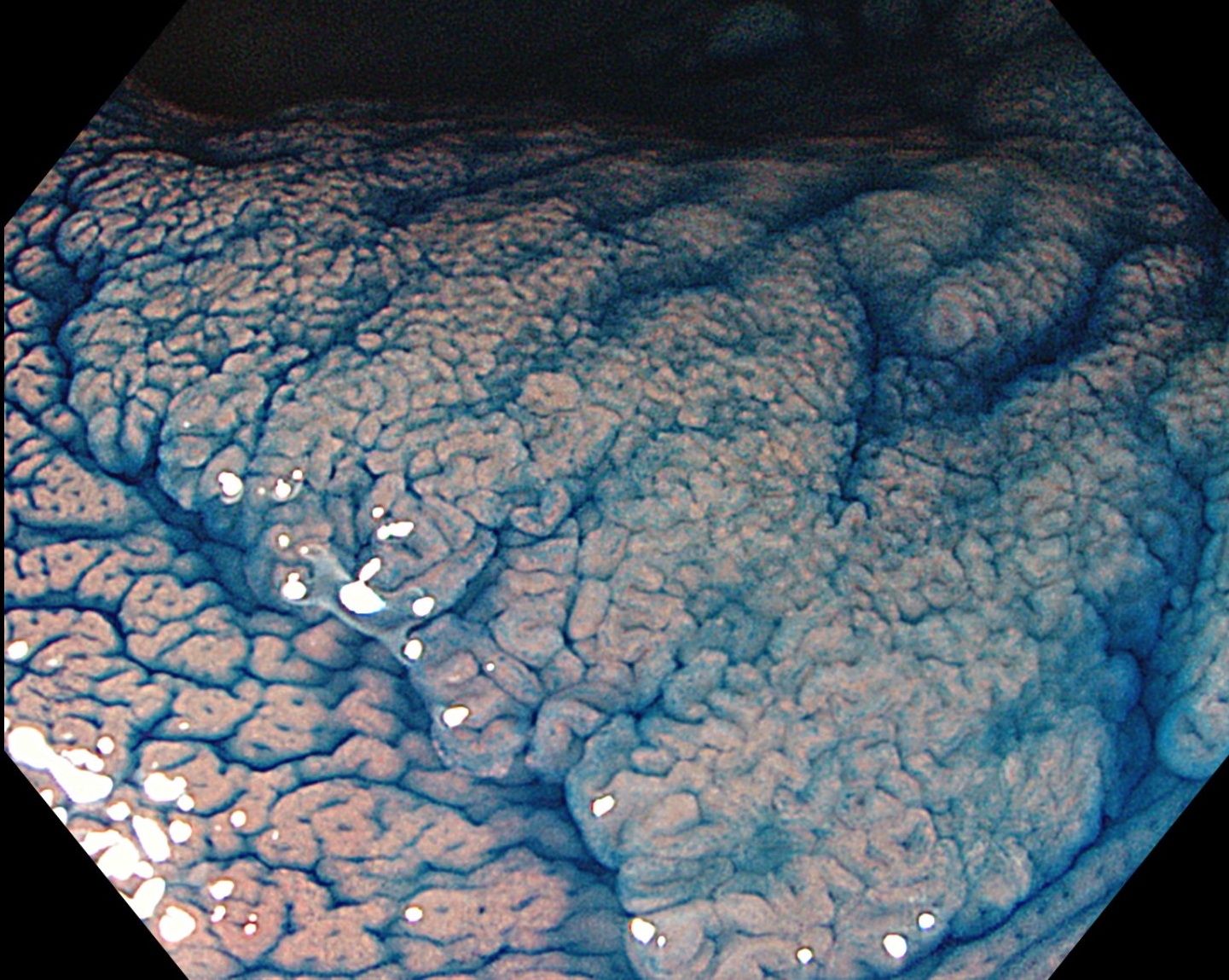
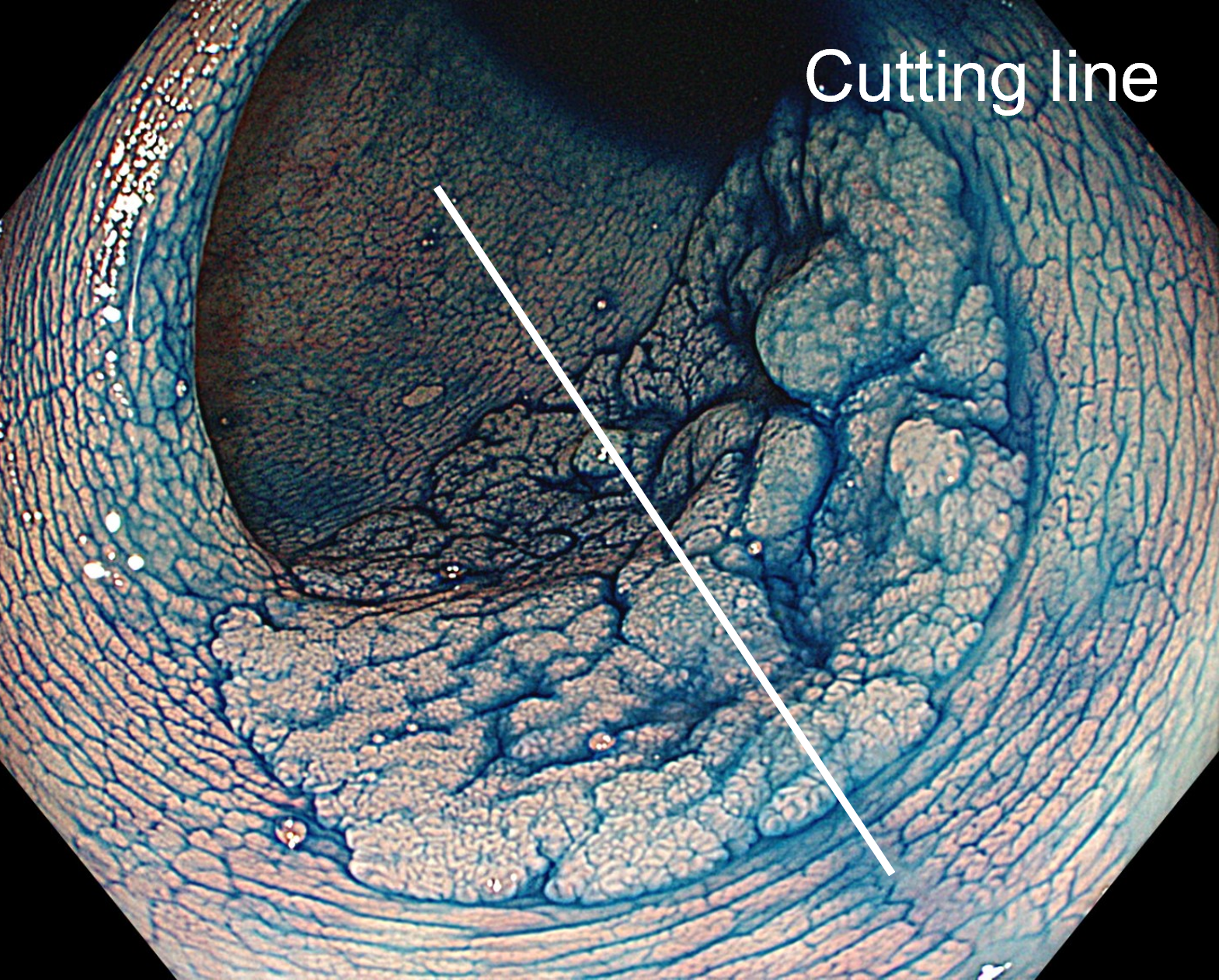
7. Chromoendoscopy
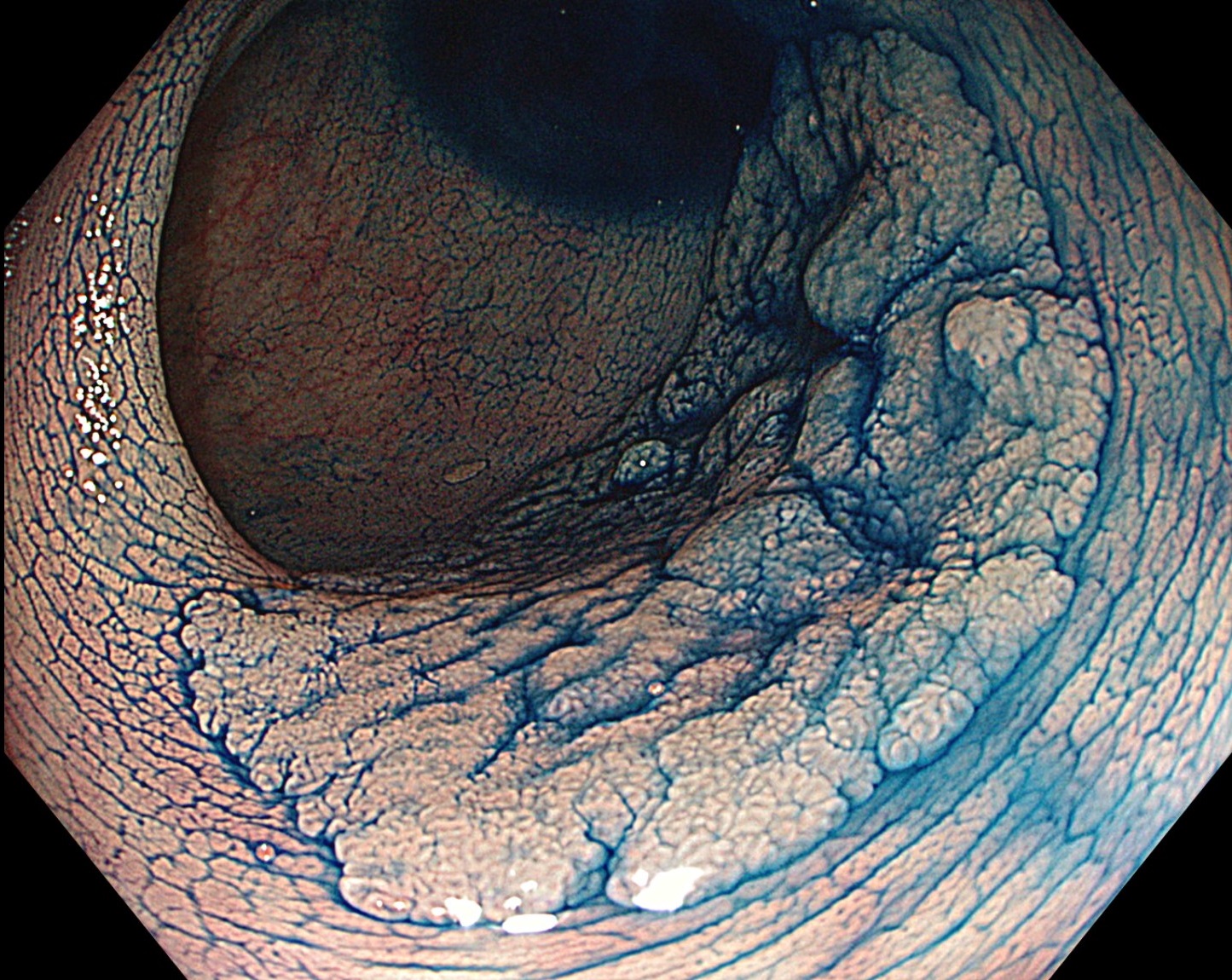
8. Chromoendoscopy
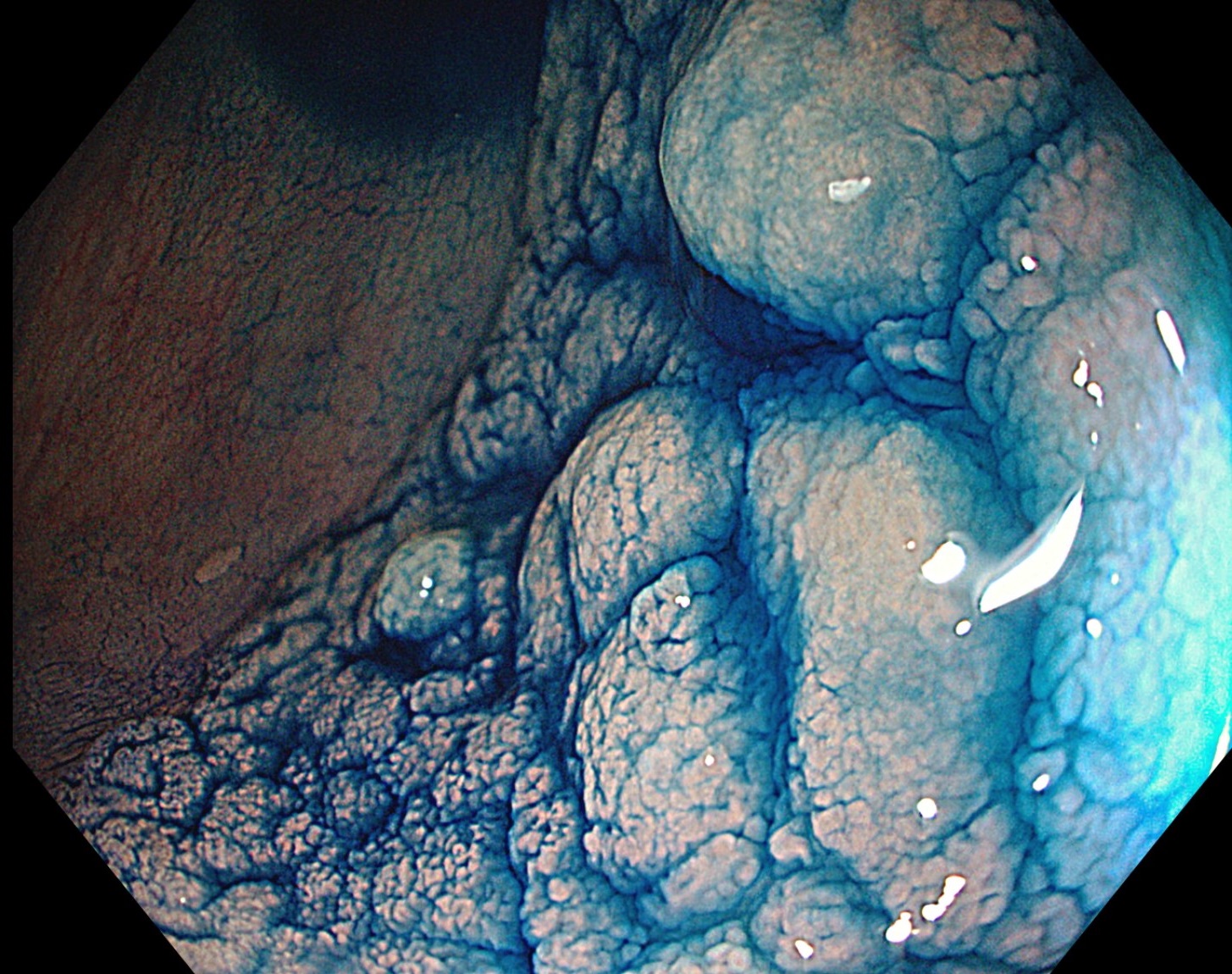
9. Chromoendoscopy
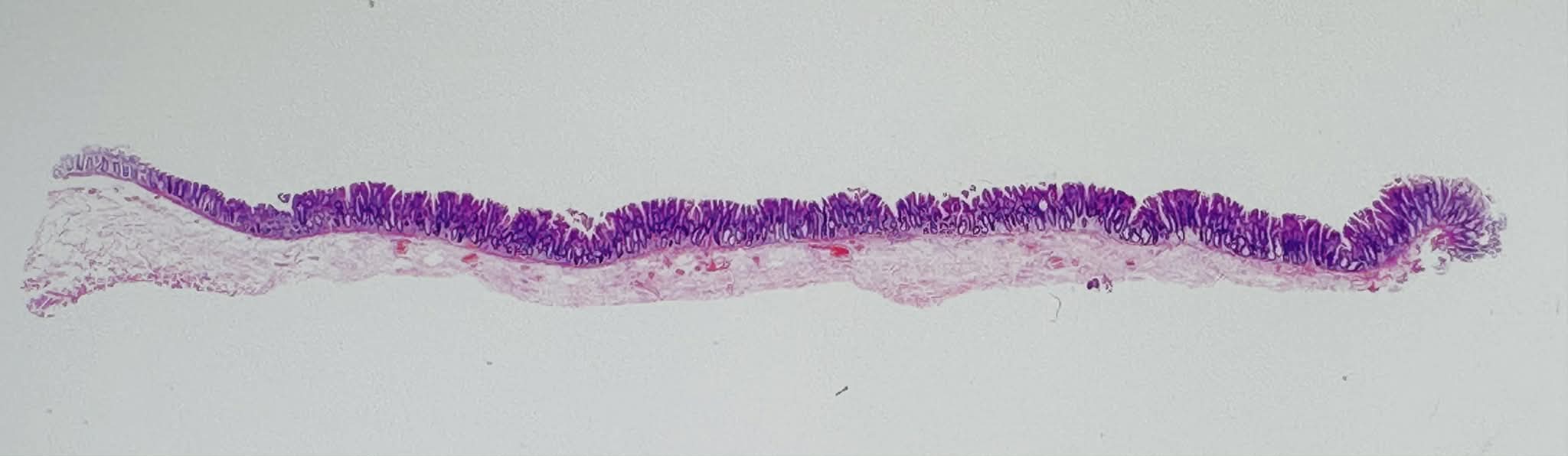
10. Pathological image
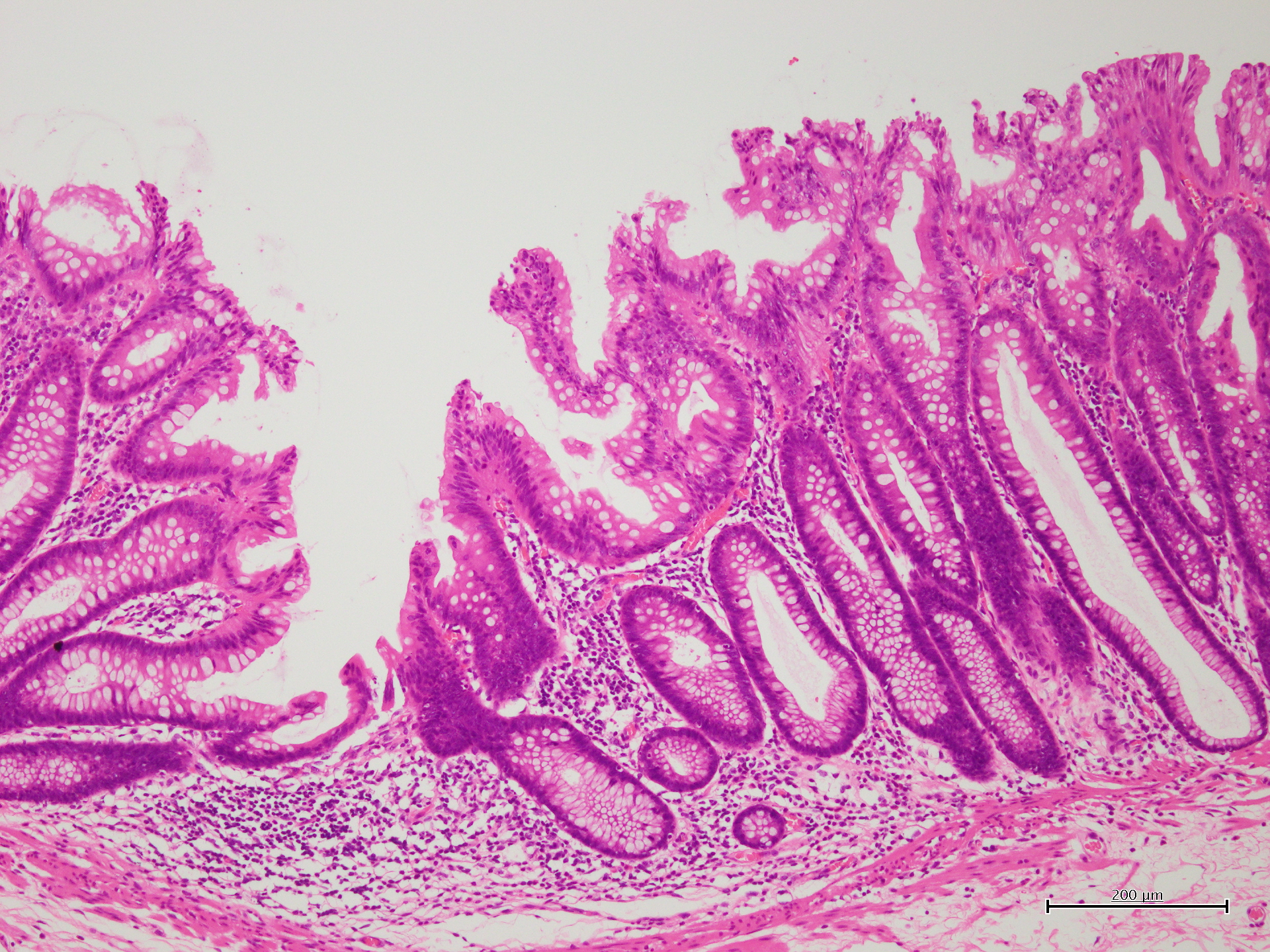
11. Pathological diagnosis
12. Pathological image
Case Video
Overall Comment
This case demonstrates a 32-mm sigmoid colon lesion that appeared macroscopically as LST-G, but was histologically diagnosed as SSL with cytological dysplasia (SuSA with traditional serrated adenoma-like appearance). On white-light imaging, the lesion was relatively subtle because it was nearly isochromatic with the surrounding mucosa, and loss of vascular transparency was an important clue to detection. TXI improved recognition of the lesion by highlighting multiple small nodular elevations of varying size. On NBI and magnifying NBI, the lesion was characterized by surface findings such as white dots and black dots, while the vascular pattern remained indistinct. Magnifying NBI-TXI further emphasized the whitish surface change, and the lesion was optically diagnosed as JNET Type 1. Indigo carmine chromoendoscopy clearly delineated the lesion extent and allowed a macroscopic diagnosis of LST-G, while magnification showed a Kudo type II pit pattern in both elevated and flat areas. This highly educational case illustrates that SuSA/SSL with cytological dysplasia may present as an LST-G-like lesion, and that careful assessment of surface morphology is essential for accurate endoscopic characterization.
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer.
- Content Type