Disclaimer
The techniques and clinical opinions presented in this material reflect the personal experience and professional judgment of the healthcare professional and do not necessarily represent the views of Olympus. This material is intended for healthcare professionals only. Users should always refer to the applicable Instructions for Use (IFU) and use Olympus products in accordance with the approved indications and local regulatory requirements. The healthcare professional presenting this material has been engaged by Olympus and compensated at fair market value for their services.
Colorectal Case 38

Yasushi Sano 1.2
MD, PhD, FJGES, and ANBIIG 3
- Clinical Professor, Kansai Medical University Osaka, Japan
- Director & Chief of Gastrointestinal Center Sano Hospital, Kobe, Japan
- Secretary, Asian Novel Bio-Imaging and Intervention Group
Scope: CF-EZ1500DI
Case: Characterization JNET 2B
Site of lesion: Lower rectum (Rs)
Patient information: M, 60s
Medical history: Melena
Other remarks: CEA 1.4 (normal)
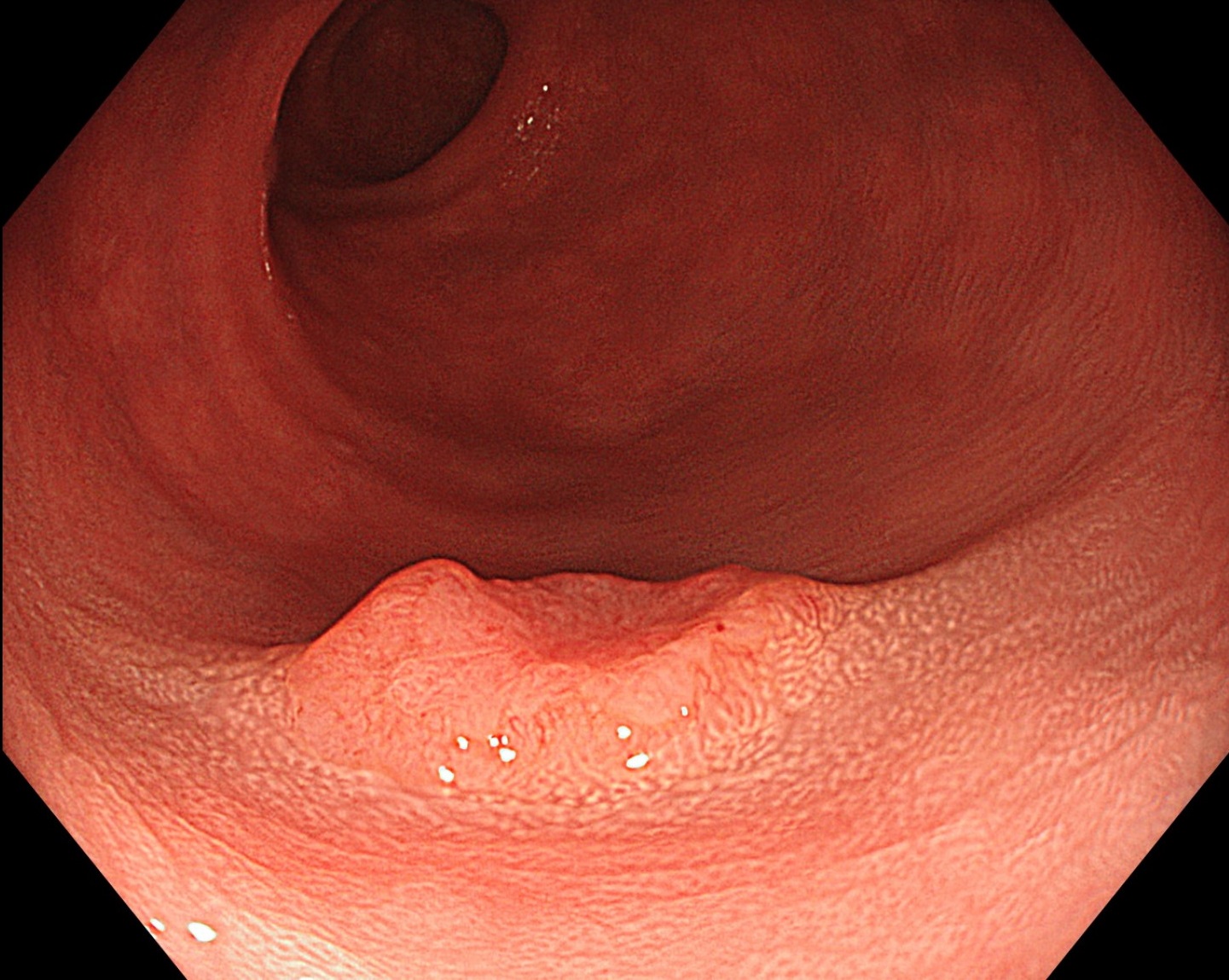
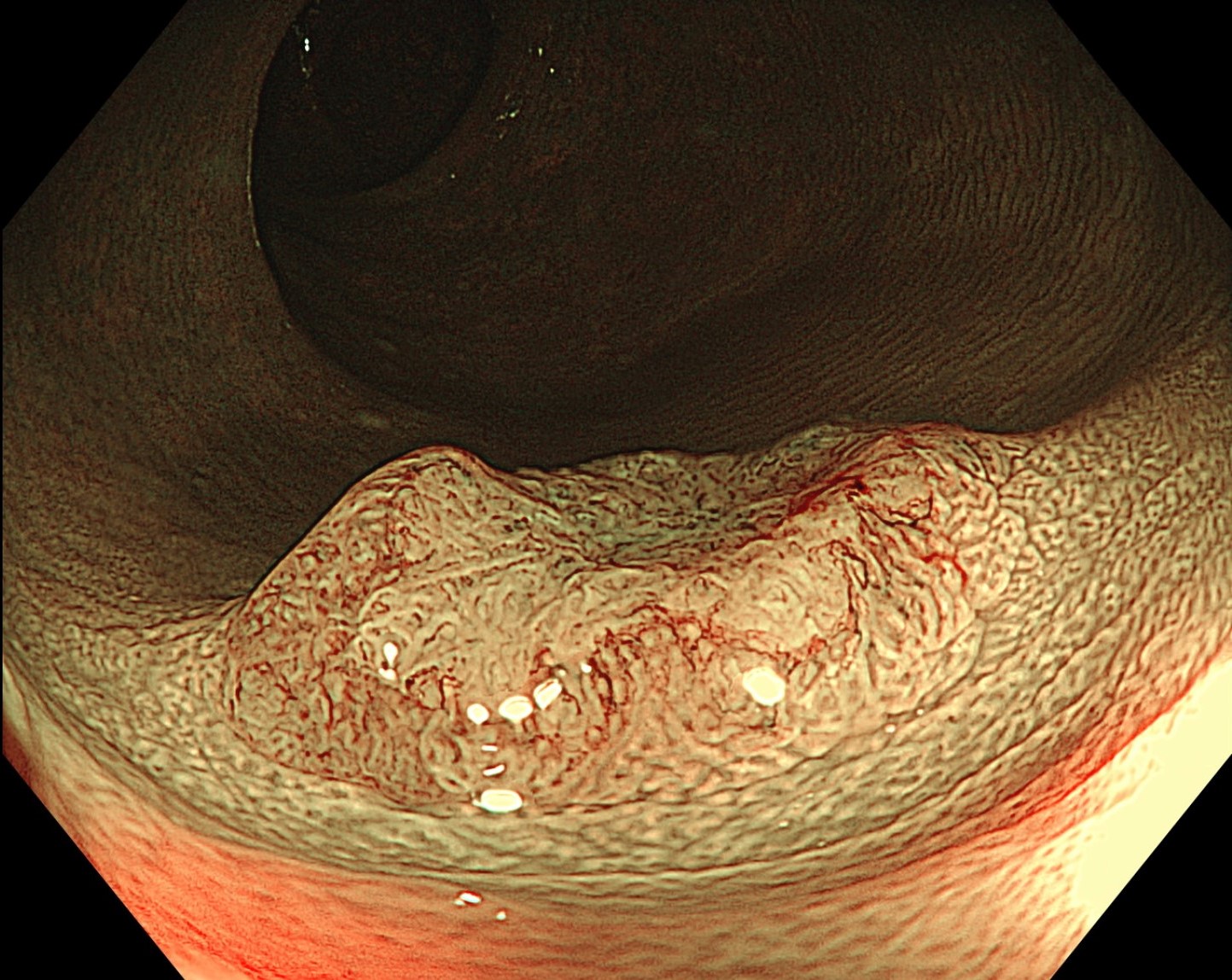
1. WLI
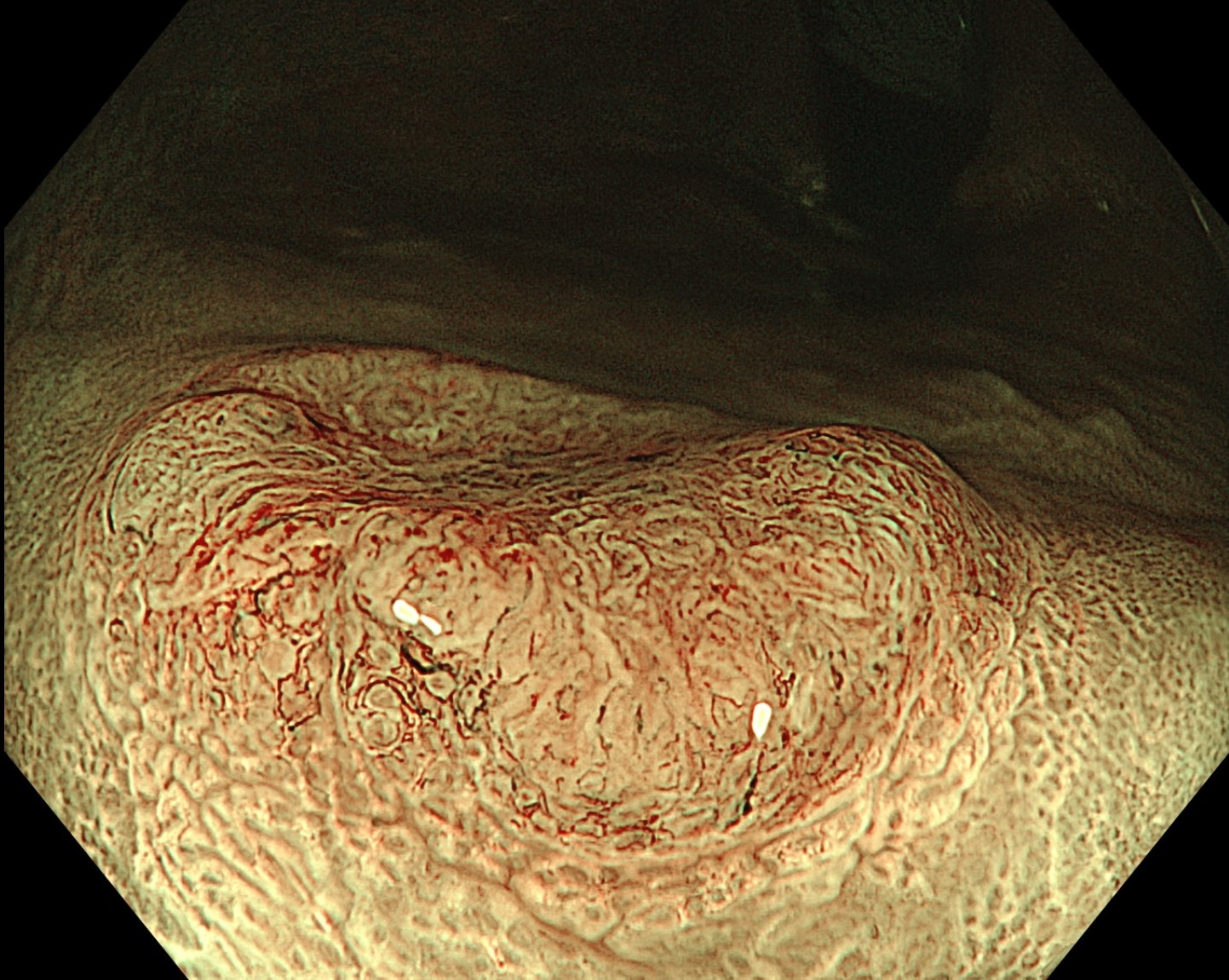
2. NBI
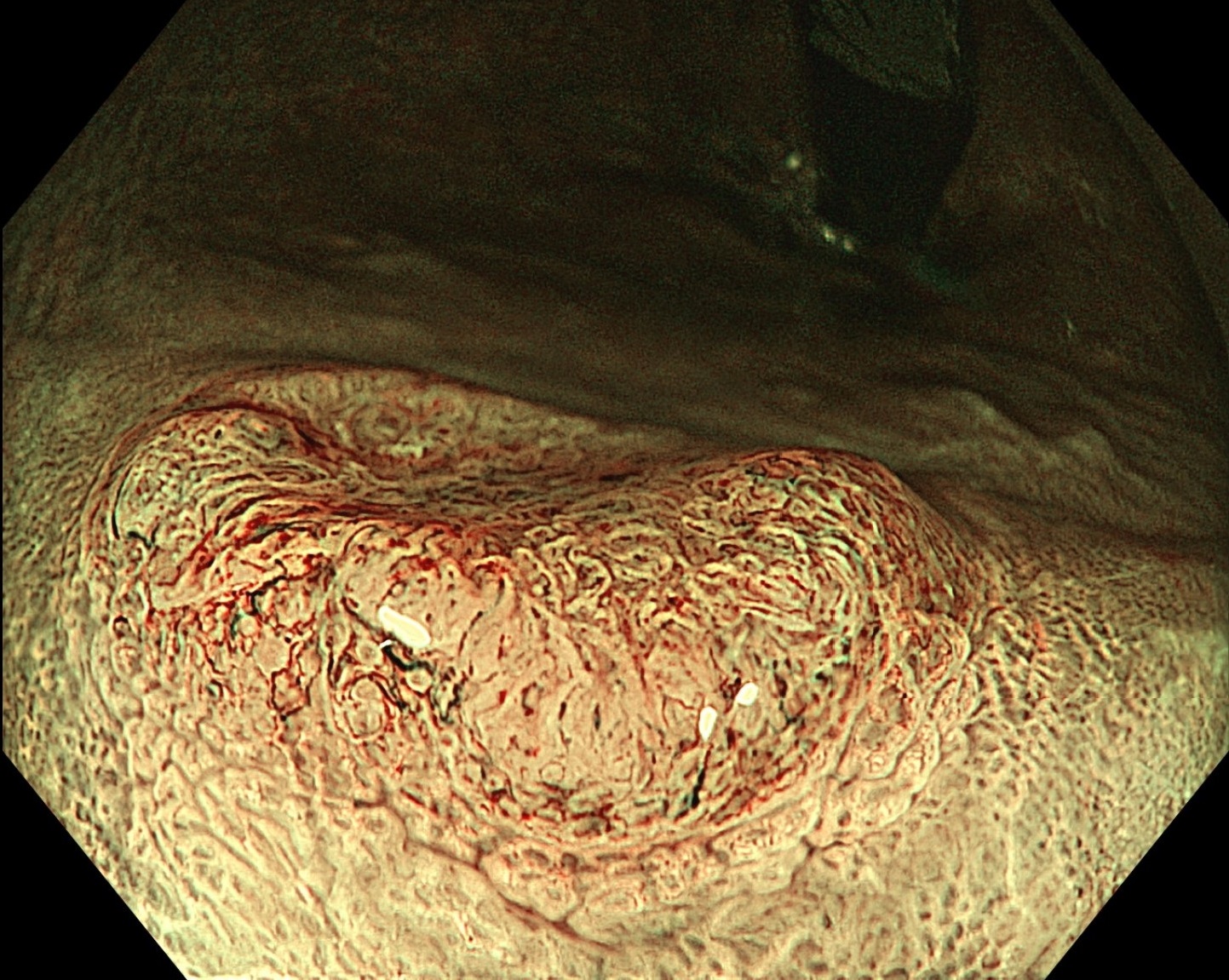
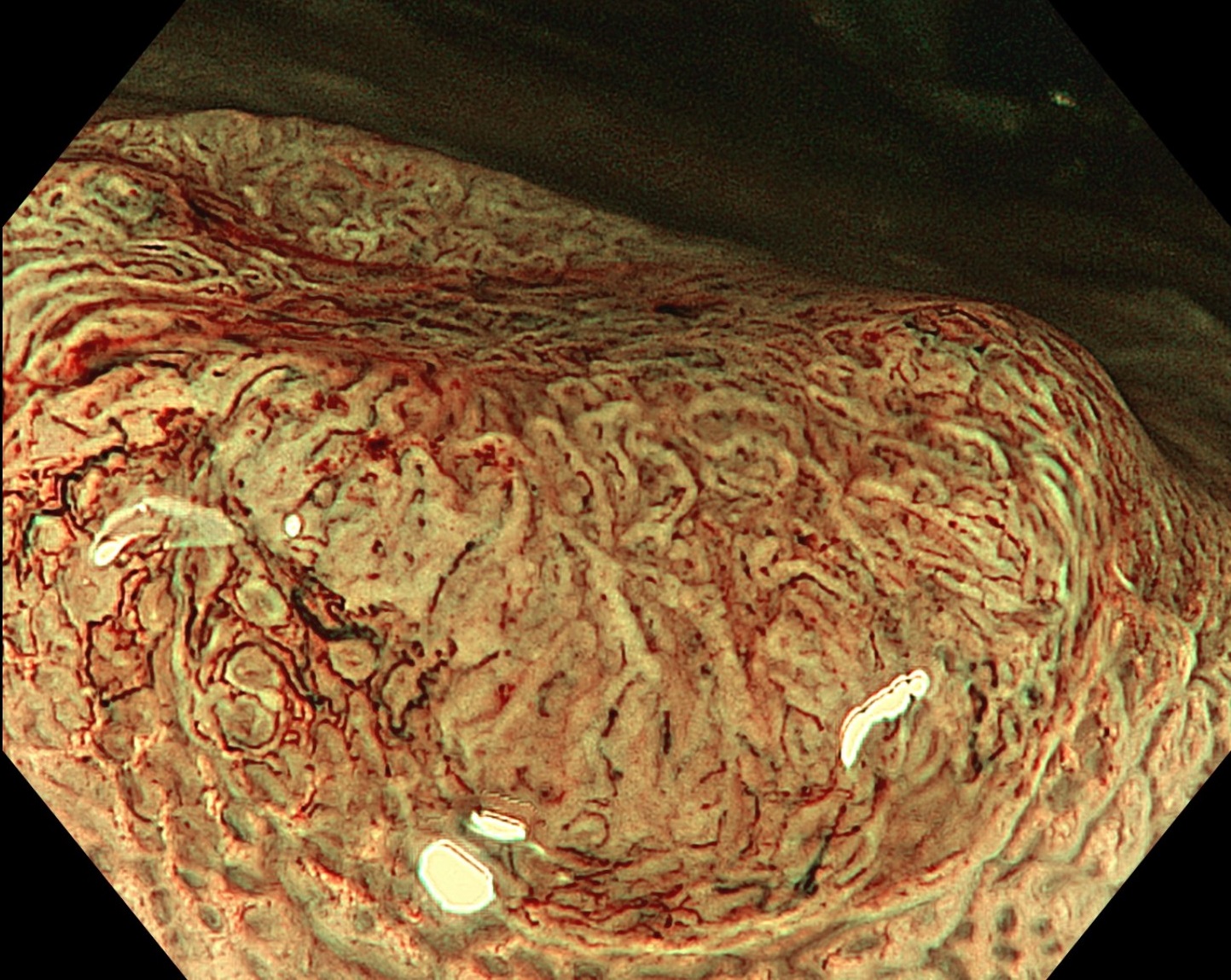
3. NBI
4. NBI+TXI
5. Zoom image NBI
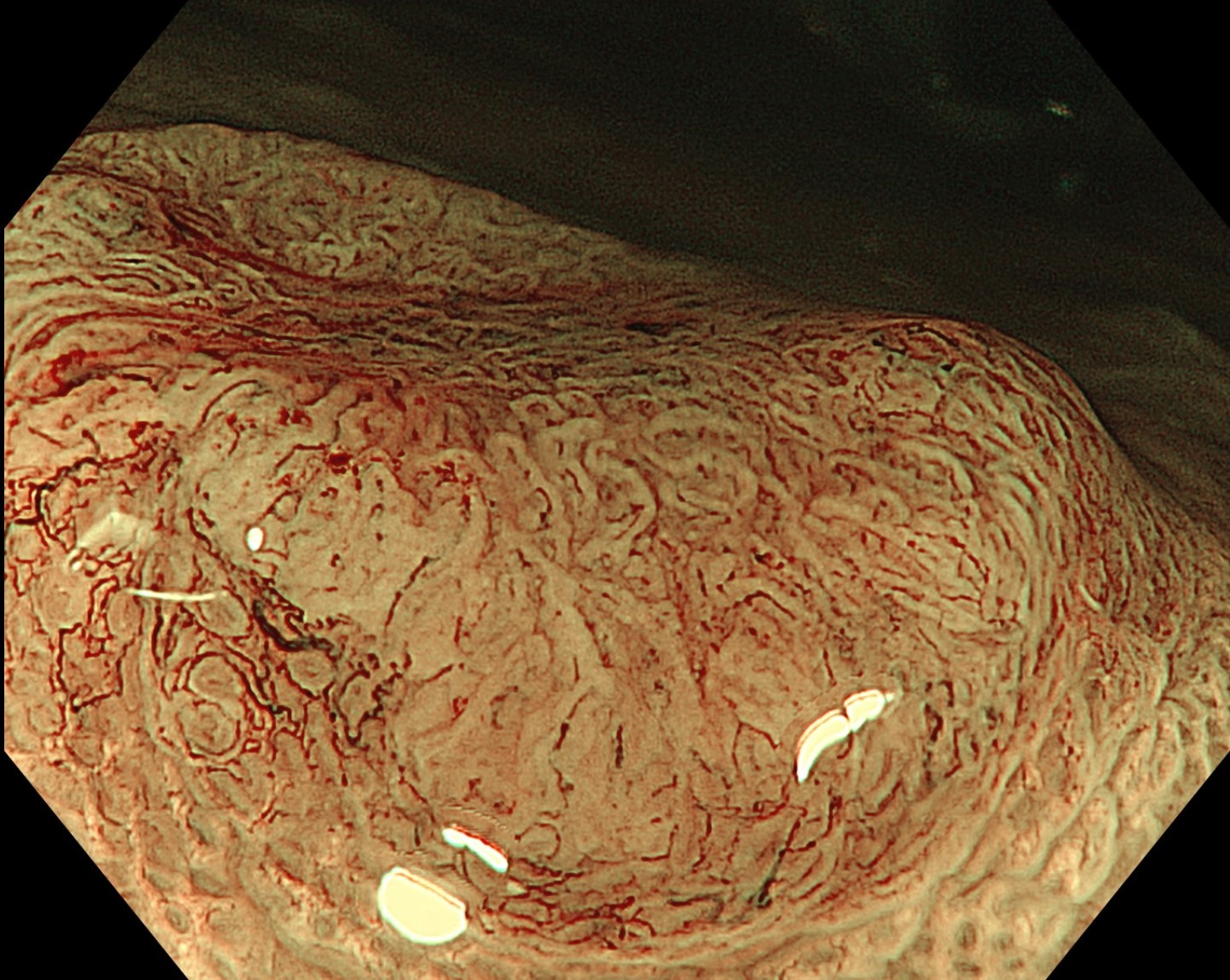
6. NBI+TXI
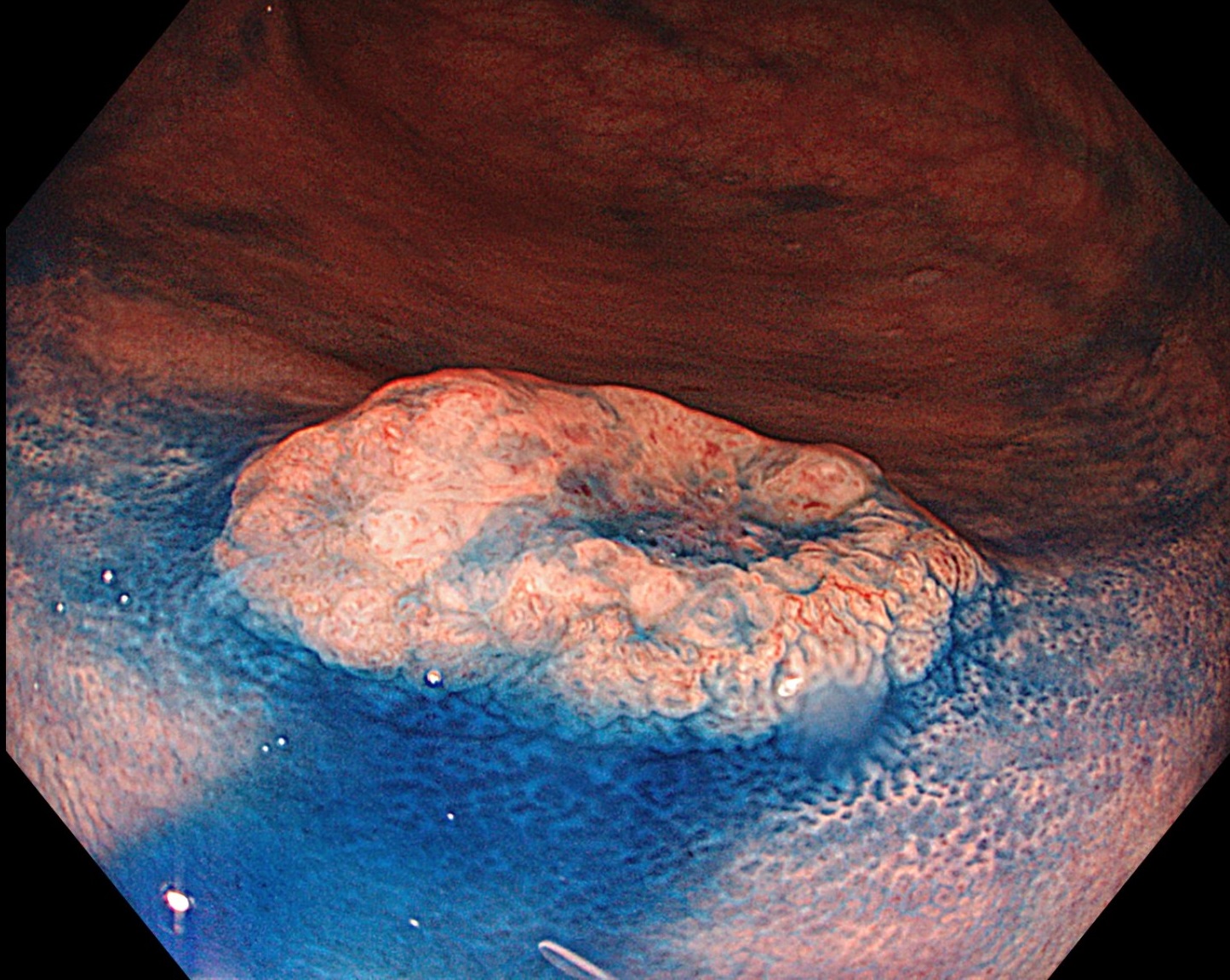
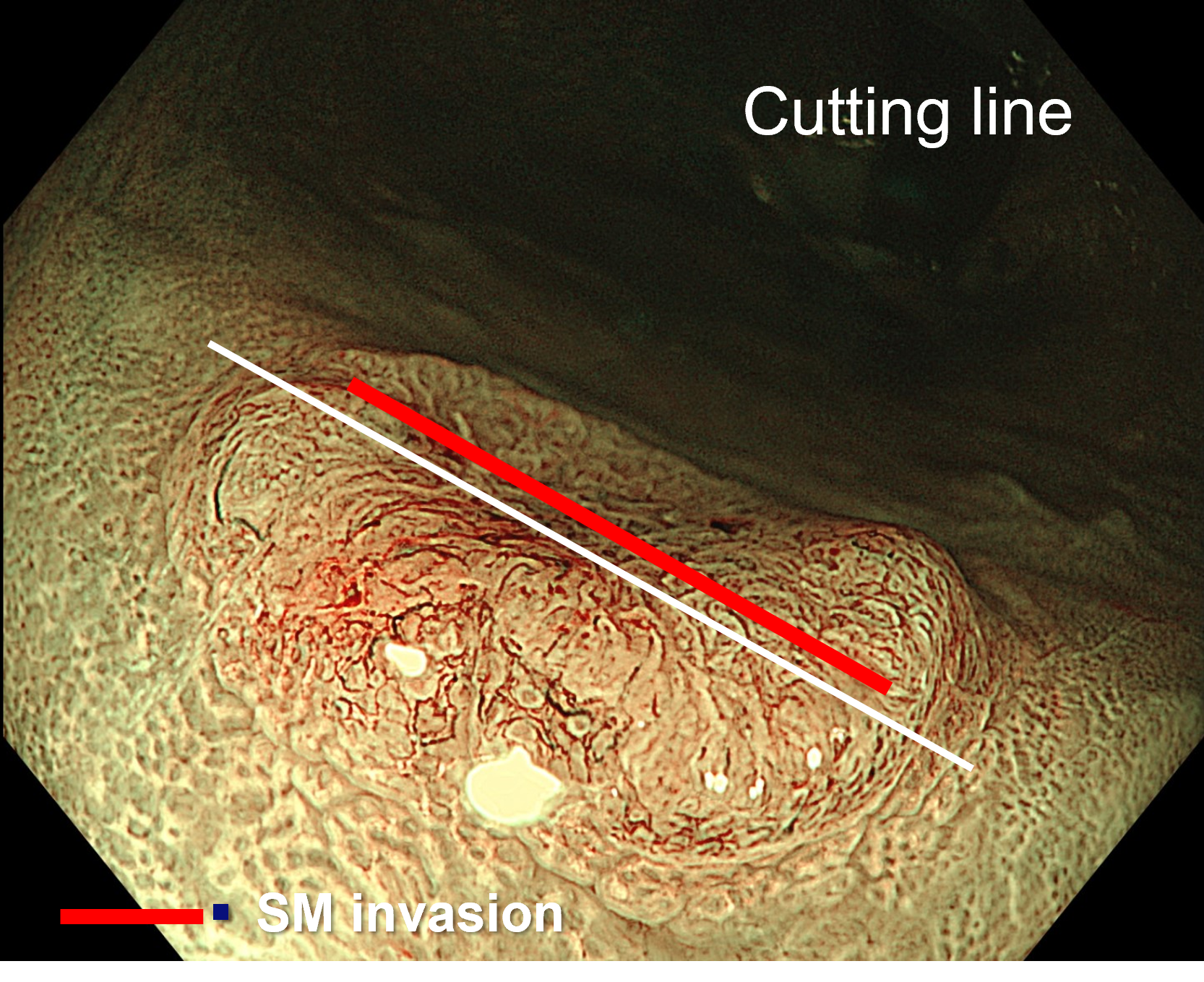
7. Chromoendoscopy
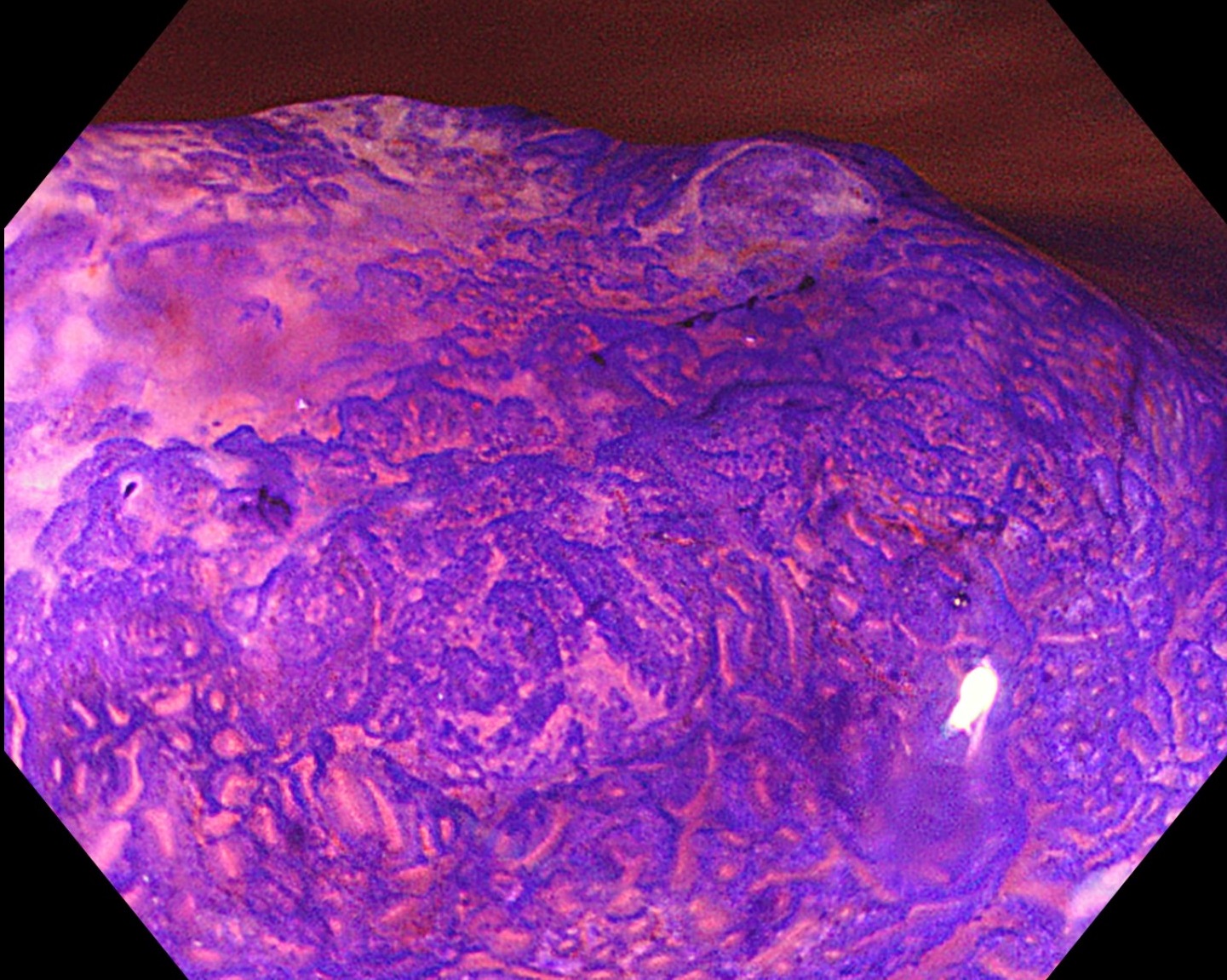
8. Chromoendoscopy
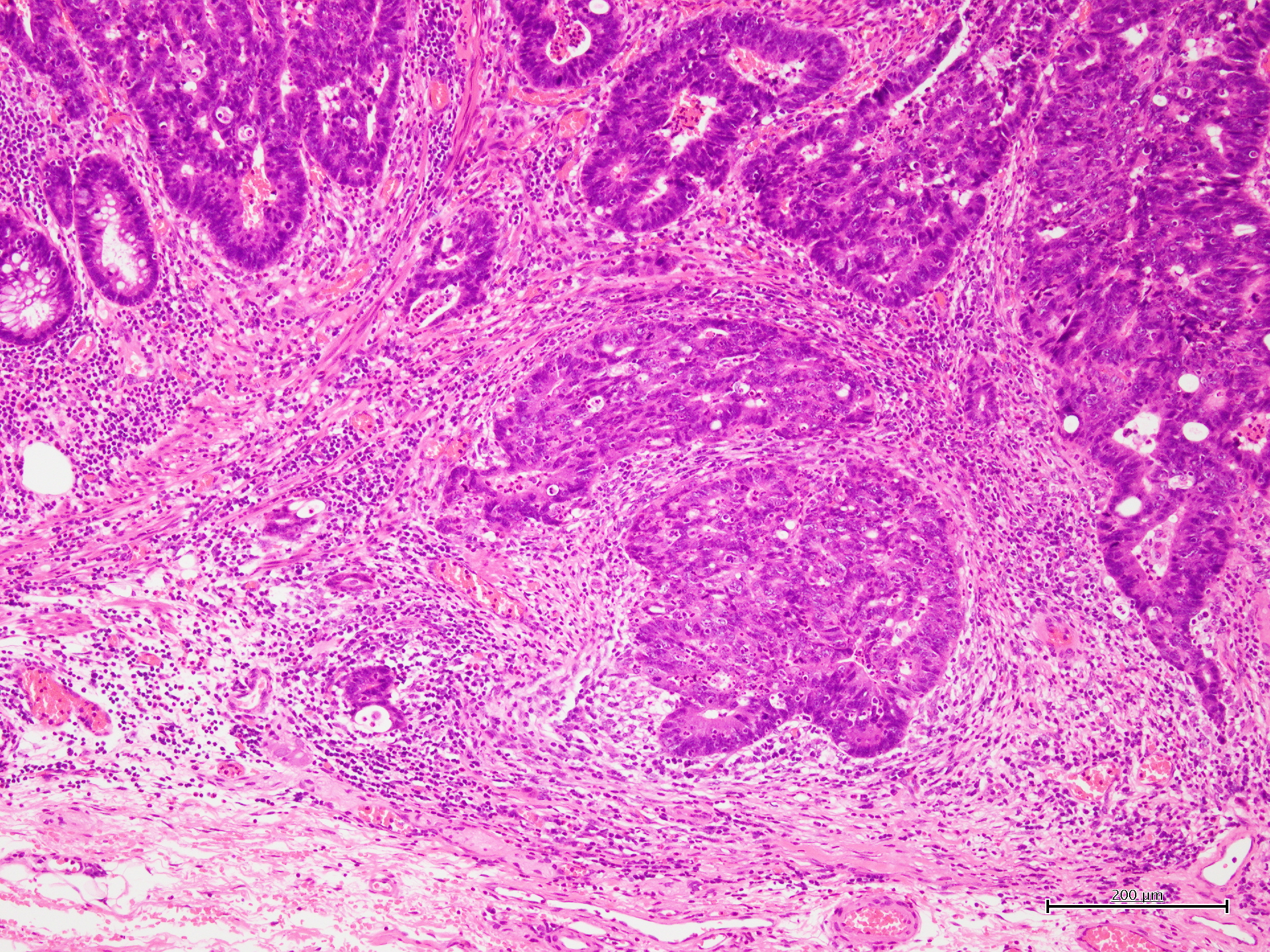
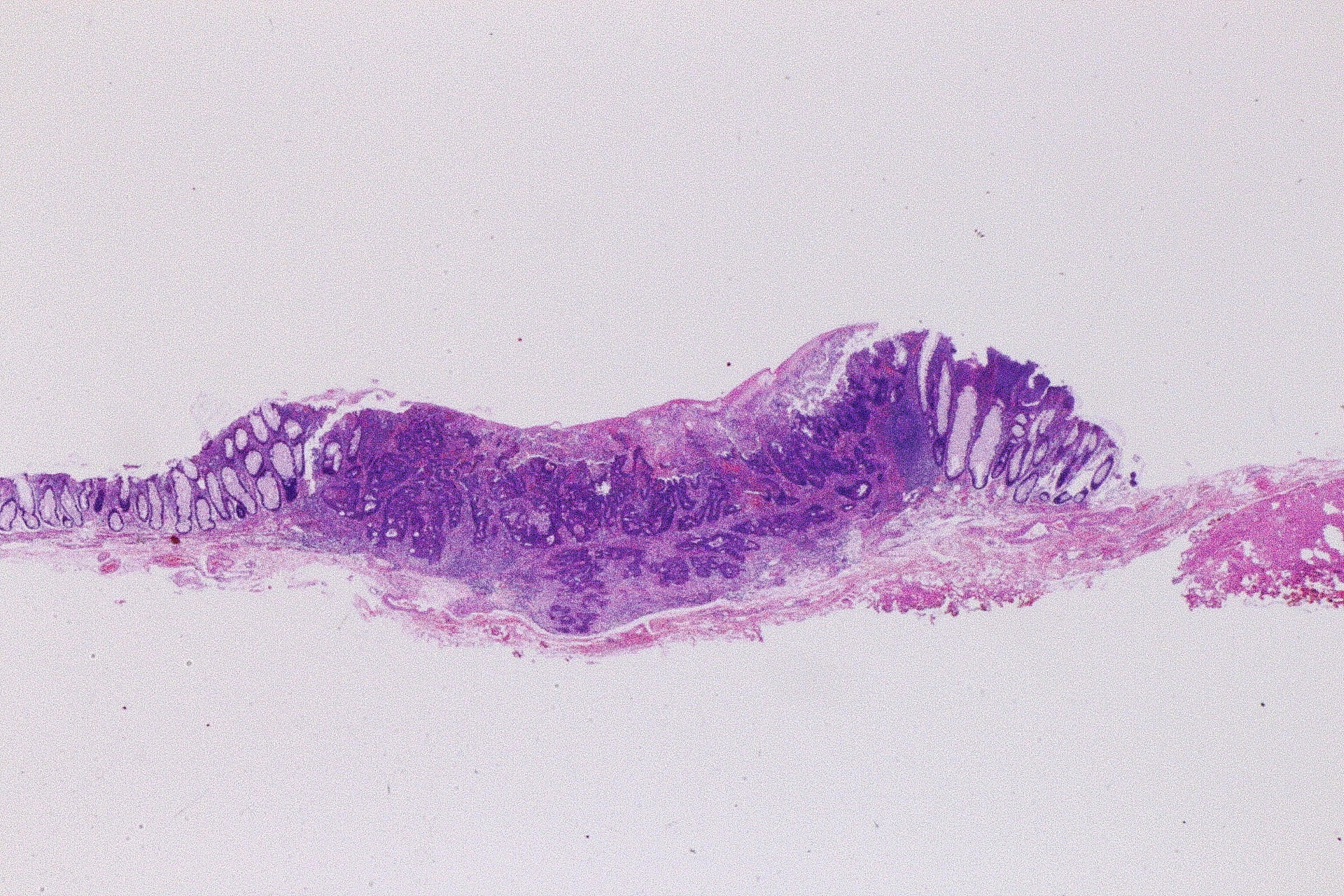
9. Pathological image
10. Pathological diagnosis
11. Pathological image
Case Video
Overall Comment
This case demonstrates an 11-mm rectal lesion (Rb) of macroscopic type 0-IIa+IIc, showing a superficially elevated component with a central depressed area and peripheral whitish change. On NBI, the depressed surface was clearly recognized, and closer observation revealed irregular vascular architecture and irregular surface pattern, leading to an optical diagnosis of JNET Type 2B. NBI-TXI made these abnormalities even more conspicuous. Magnifying NBI showed that the JNET Type 2B area extended over at least 3 mm, while magnifying NBI-TXI demonstrated white opaque substance (WOS), a finding characteristic of carcinoma. Indigo carmine chromoendoscopy further highlighted the irregular surface morphology, and crystal violet chromoendoscopy revealed a severely irregular Kudo type VI pit pattern with a positive invasive pattern, strongly suggesting SM2 or deeper submucosal invasion. Based on these findings, PAEM (peranal endoscopic myectomy) was performed. Histopathology confirmed adenocarcinoma (tub1+tub2), pT1b (SM1506 μm), BD1, ly0, v0, pHM0, pVM0. After discussion with the patient, the lesion has been managed with follow-up, and no recurrence has been observed. This highly educational case highlights the importance of integrating morphology, vascular and surface pattern analysis, WOS, and pit pattern assessment for accurate invasion-depth diagnosis in small rectal lesions.
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer.
- Content Type