Disclaimer
The techniques and clinical opinions presented in this material reflect the personal experience and professional judgment of the healthcare professional and do not necessarily represent the views of Olympus. This material is intended for healthcare professionals only. Users should always refer to the applicable Instructions for Use (IFU) and use Olympus products in accordance with the approved indications and local regulatory requirements. The healthcare professional presenting this material has been engaged by Olympus and compensated at fair market value for their services.
Colorectal Case 37

Yasushi Sano 1.2
MD, PhD, FJGES, and ANBIIG 3
- Clinical Professor, Kansai Medical University Osaka, Japan
- Director & Chief of Gastrointestinal Center Sano Hospital, Kobe, Japan
- Secretary, Asian Novel Bio-Imaging and Intervention Group
Scope: CF-XZ1200I
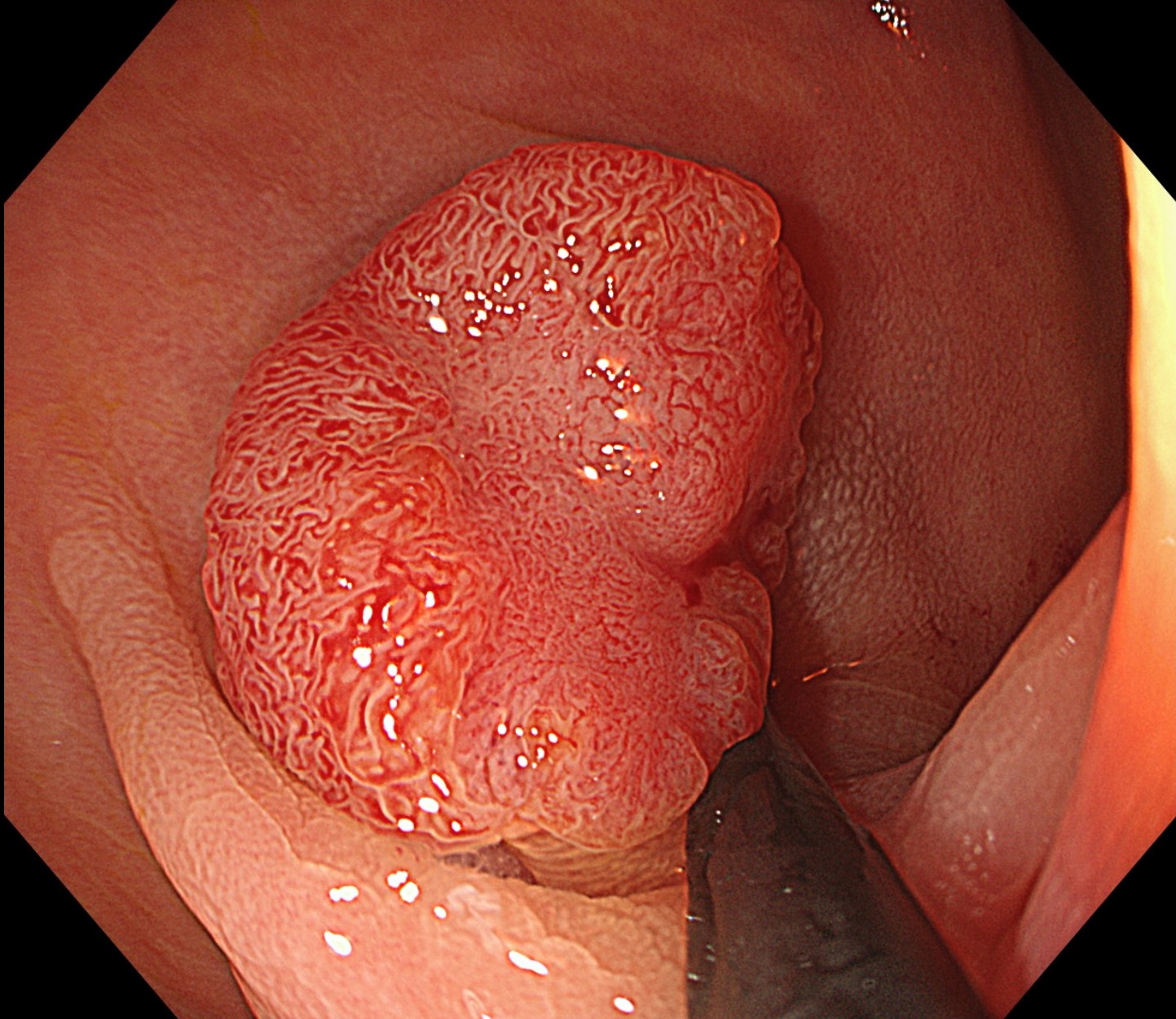
Case: Characterization JNET 2B
Site of lesion: Lower rectum (Rs)
Patient information: M, 50s
Medical history: Melena
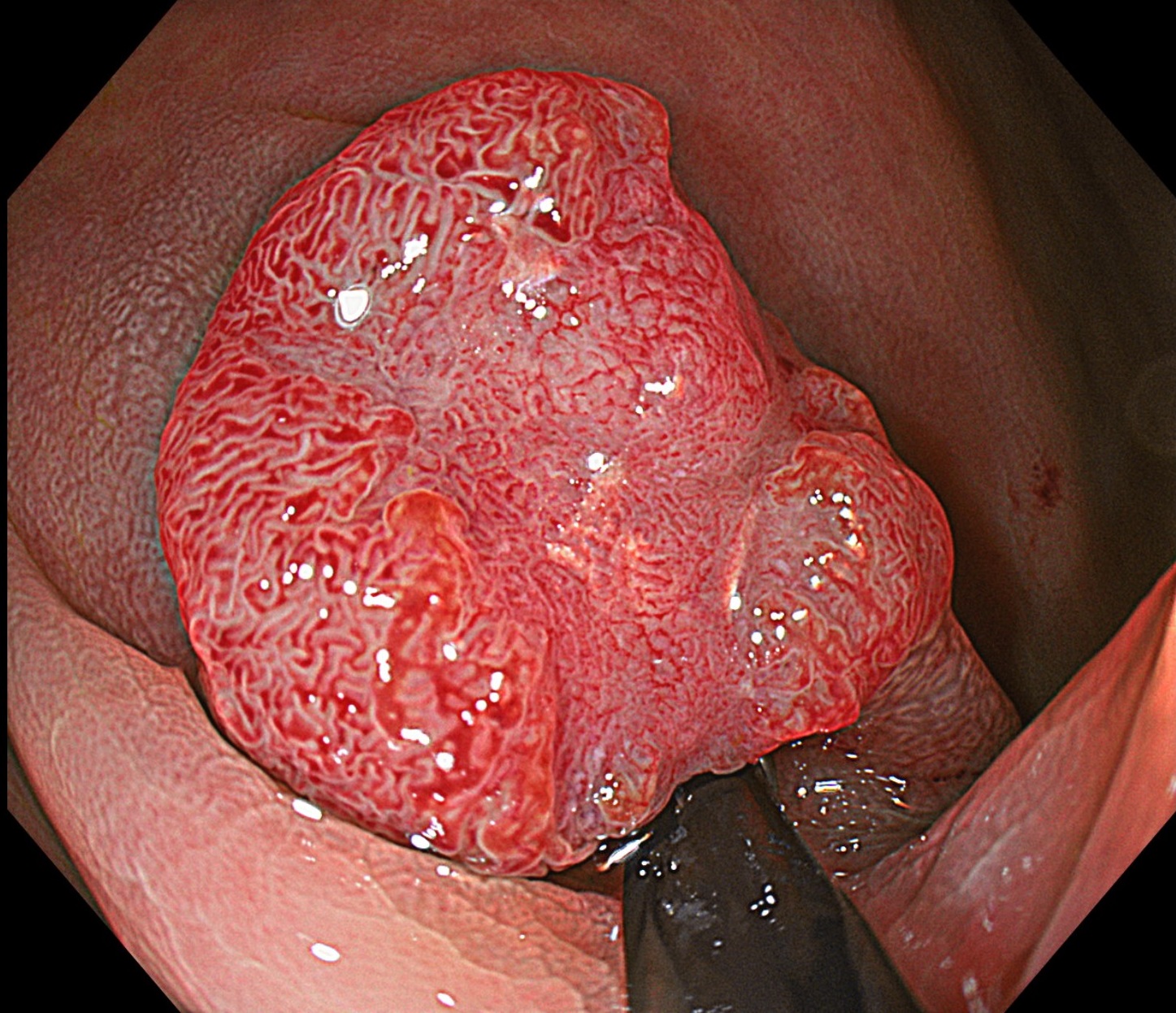
1. WLI
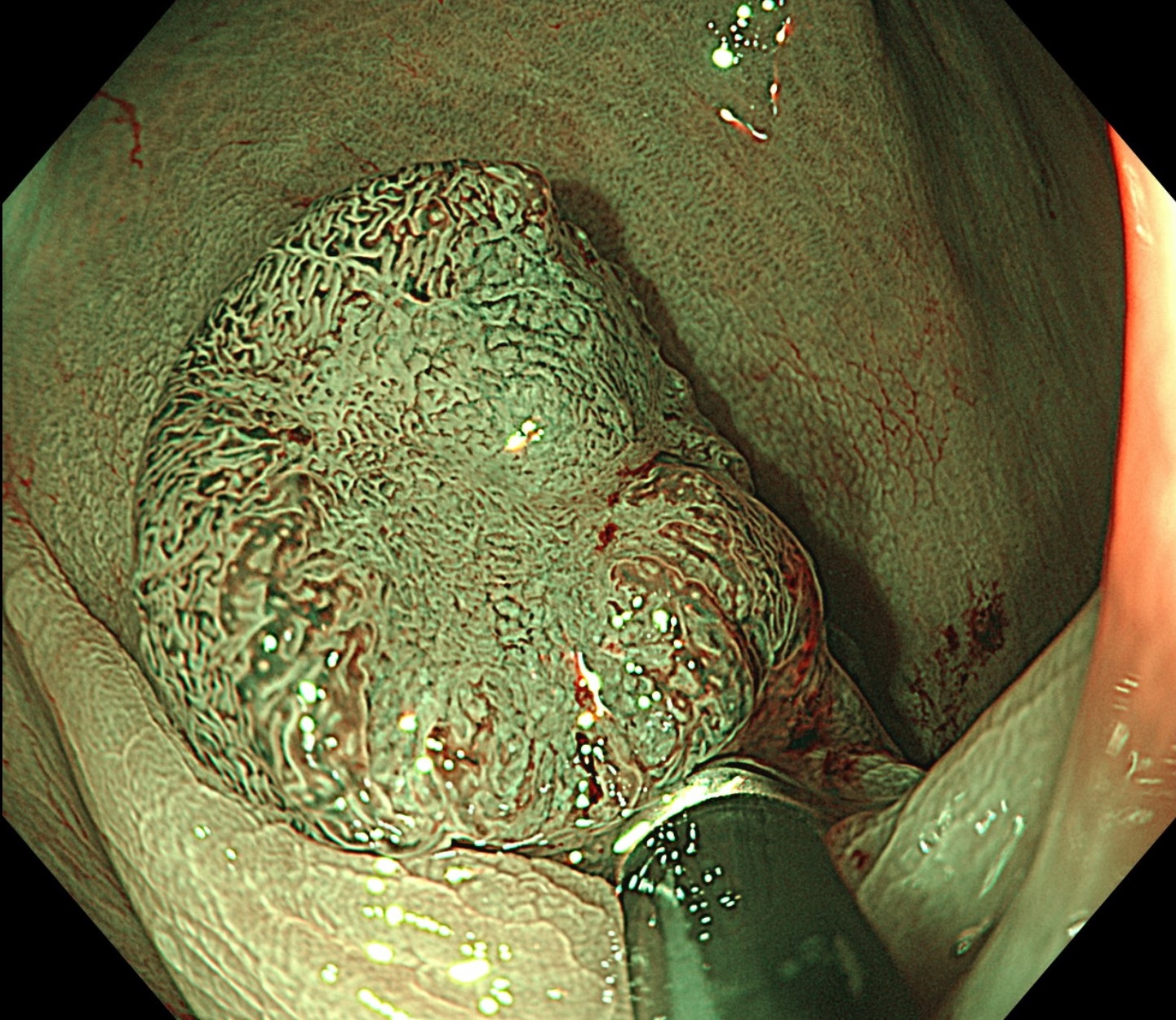
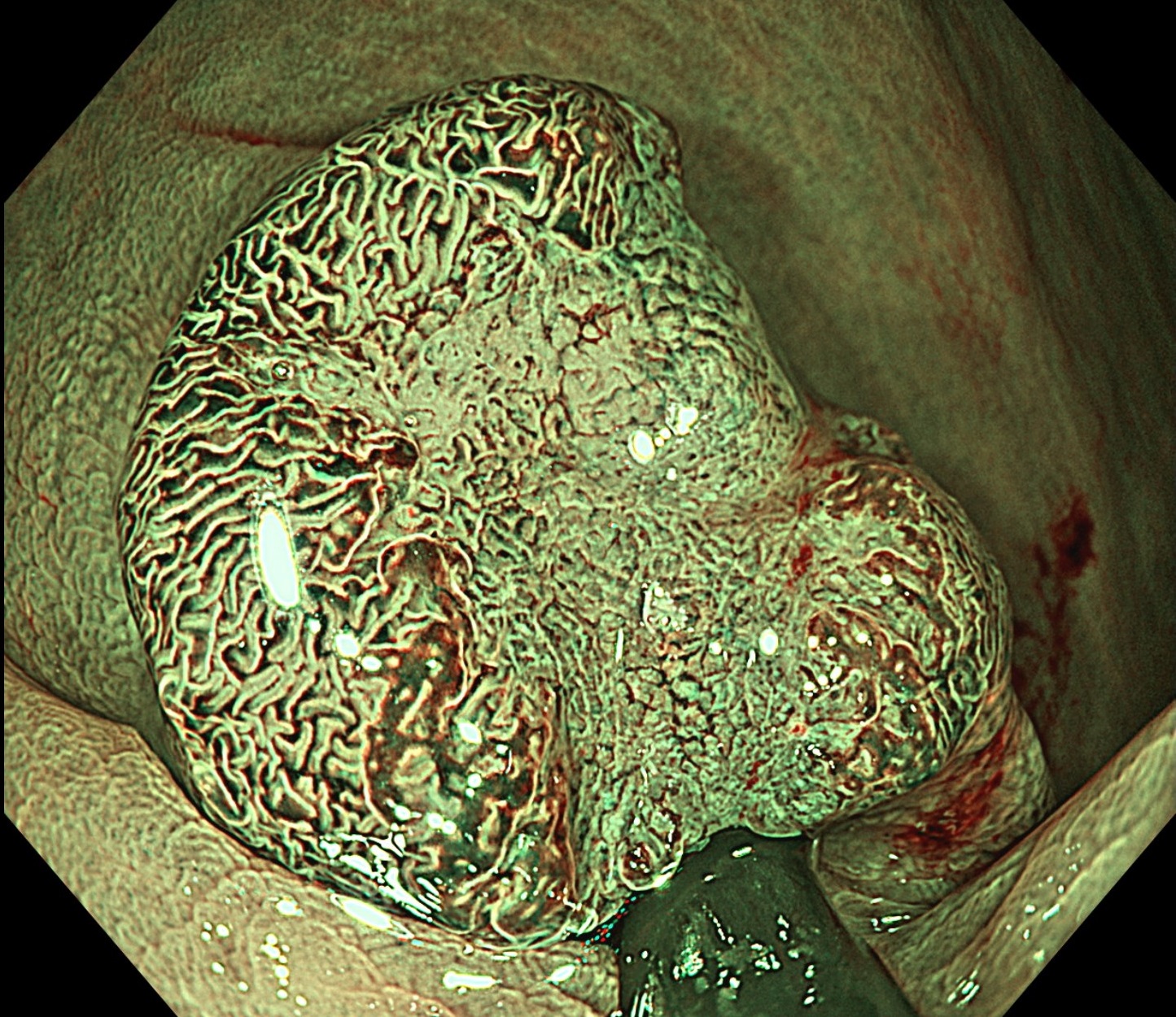
2. TXI
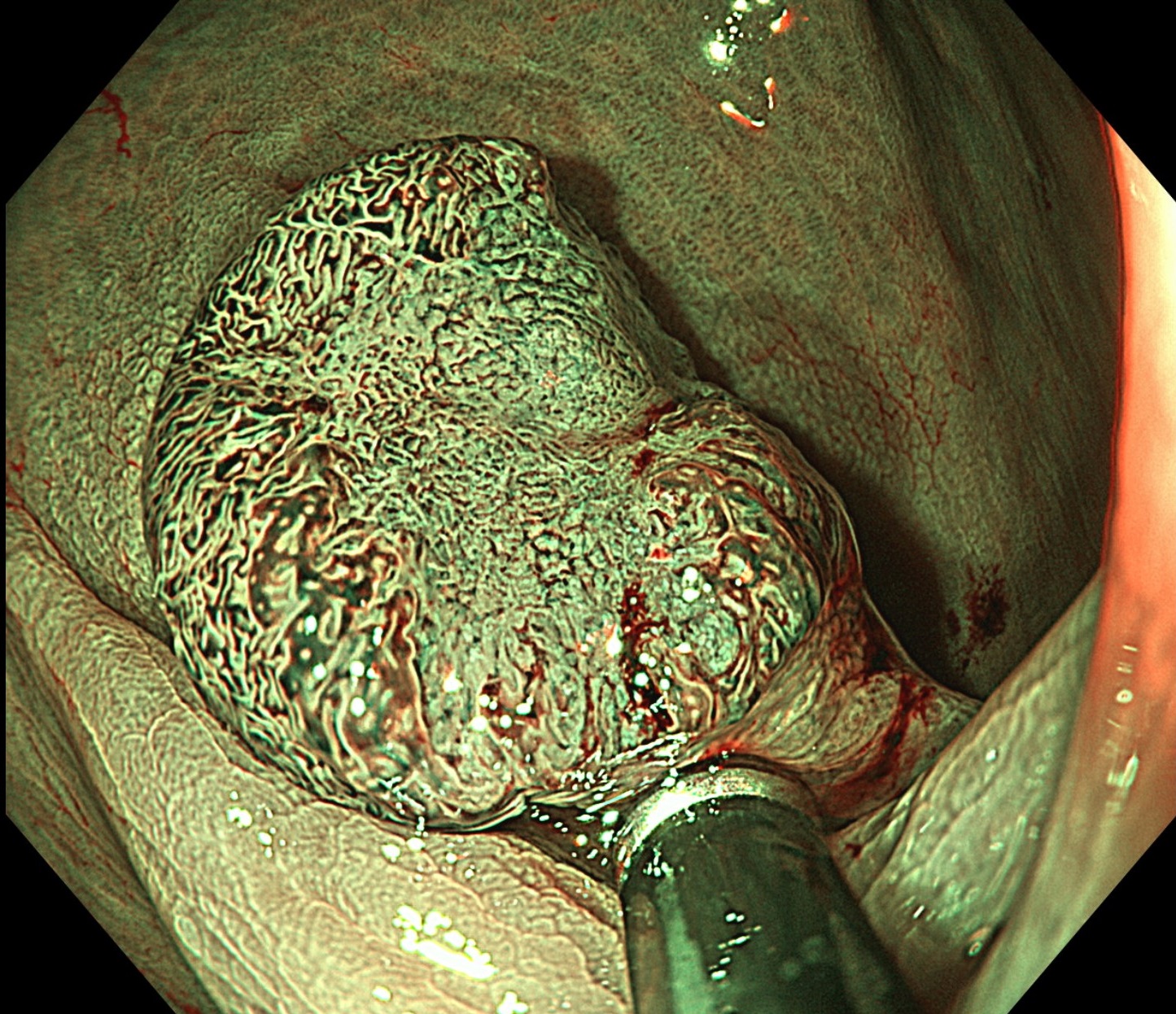
3. NBI
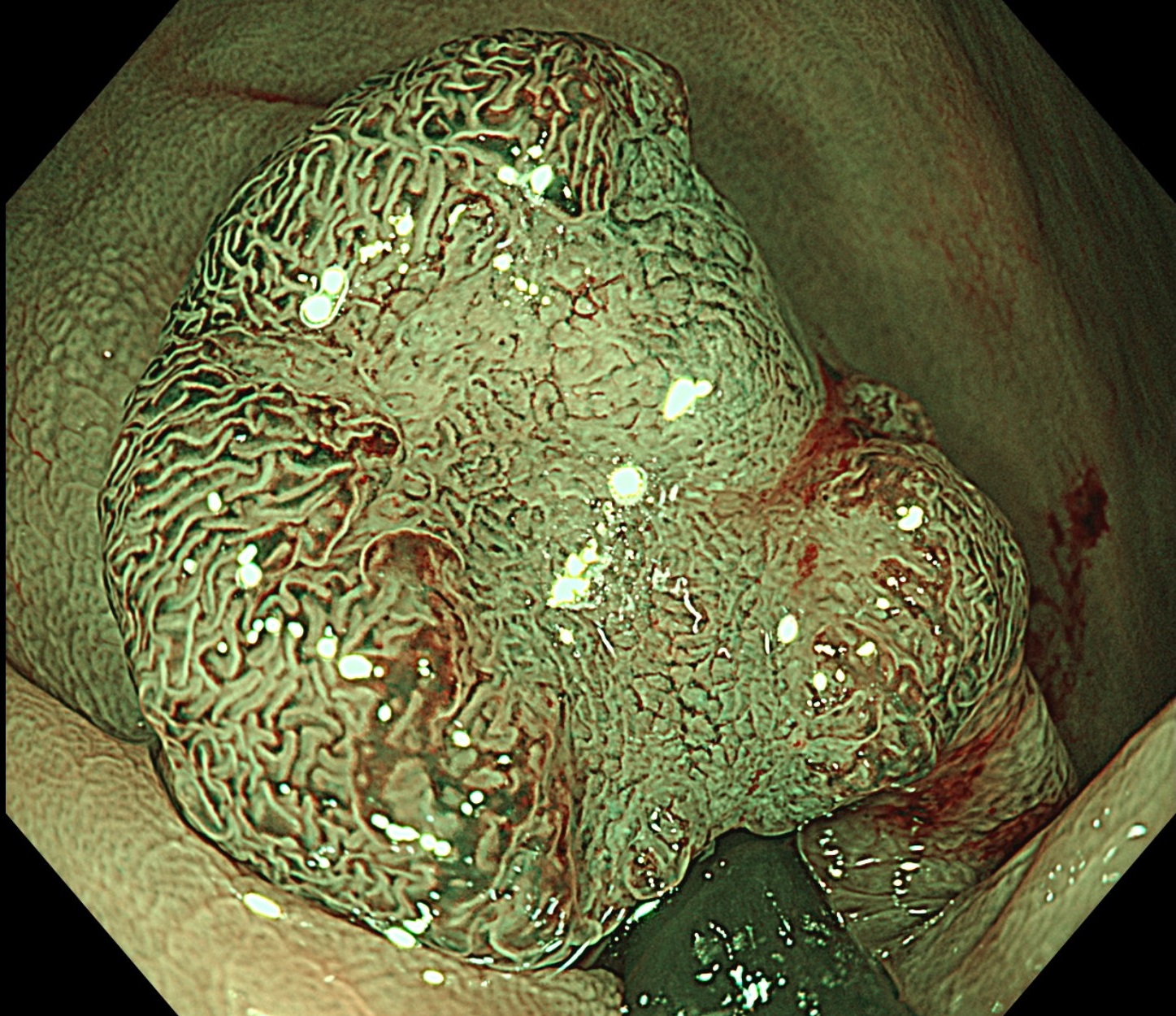
4. NBI+TXI
5. Zoom image NBI
6. NBI+TXI
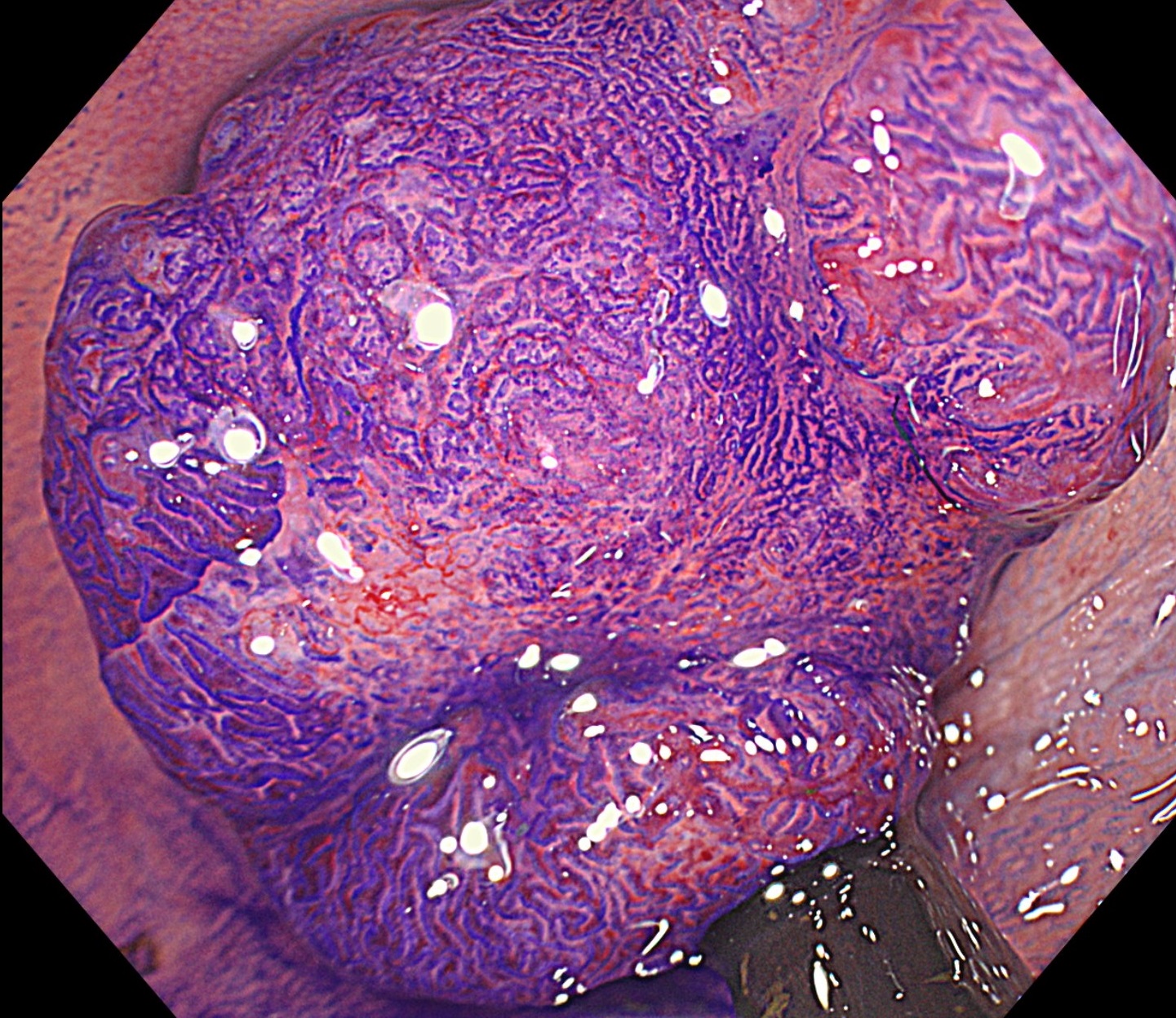
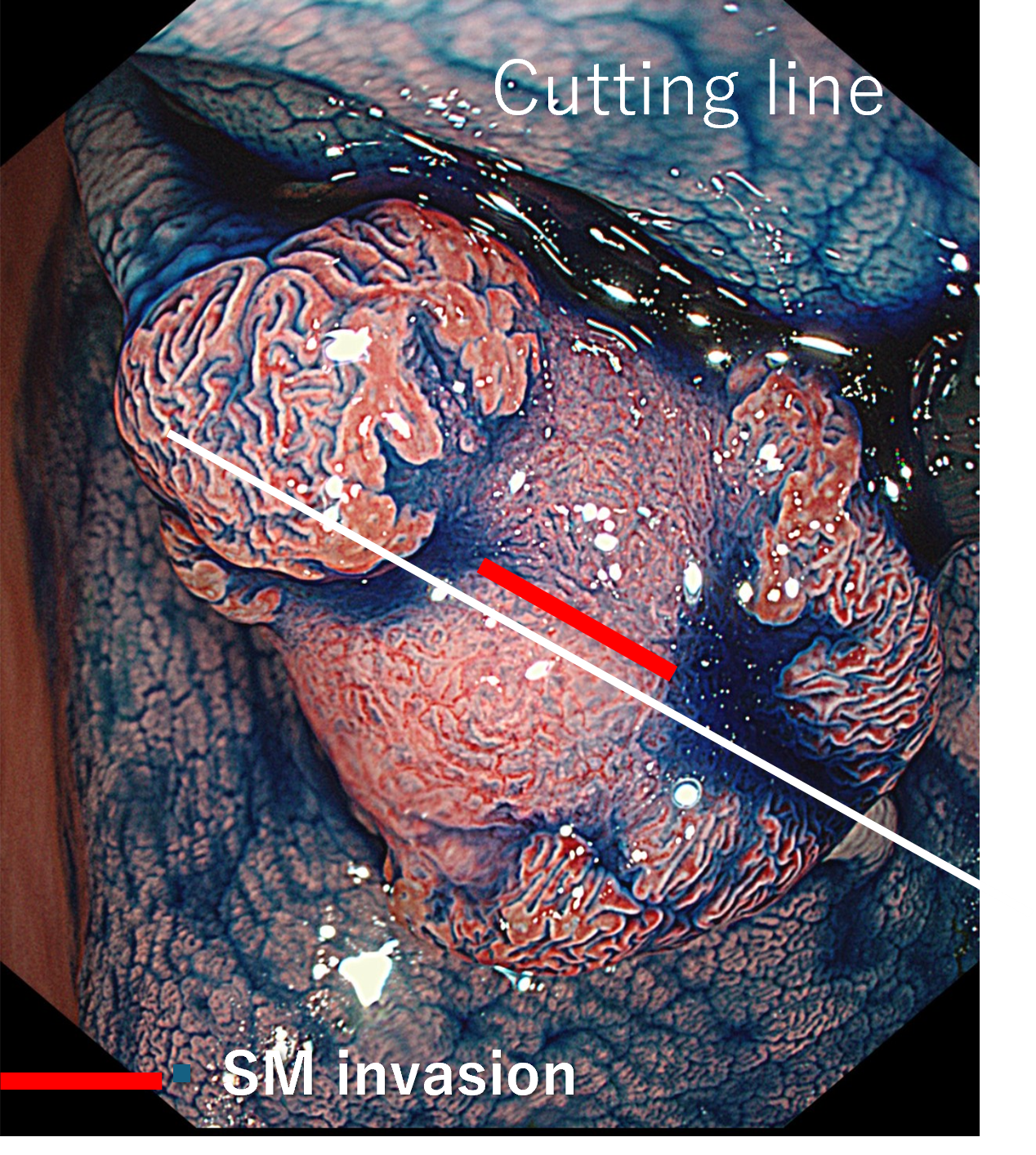
7. Chromoendoscopy
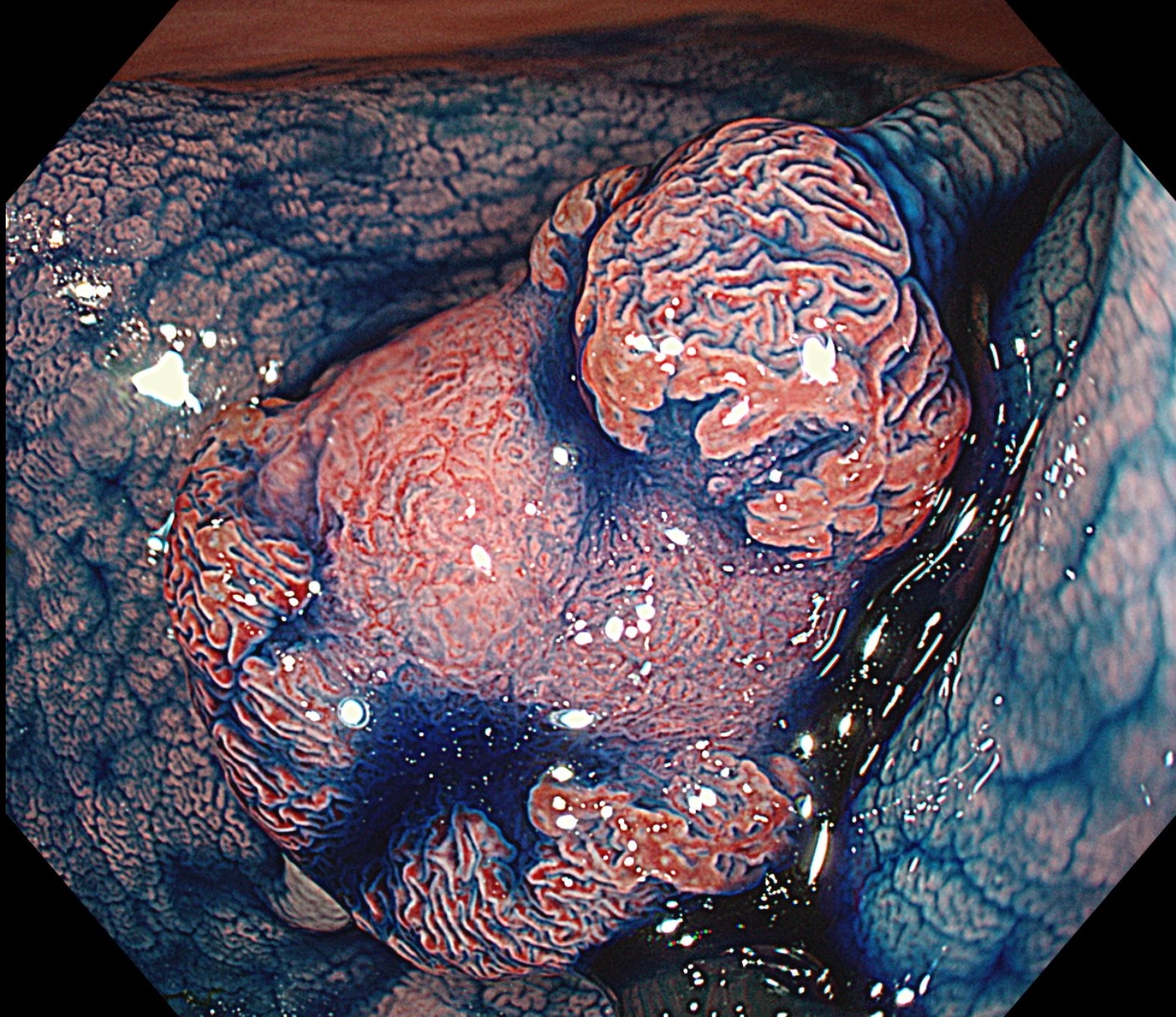
8. Chromoendoscopy
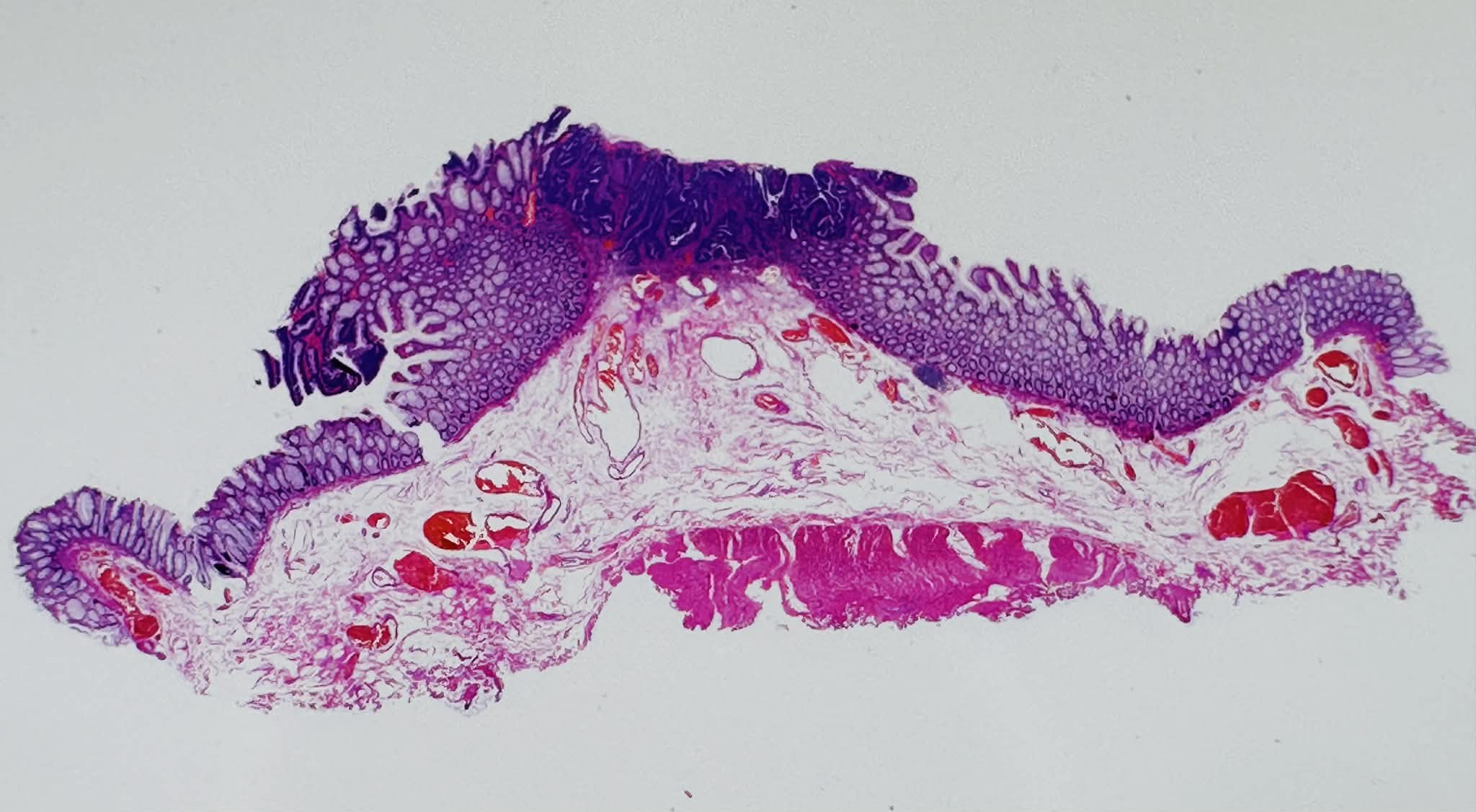
9. Pathological image
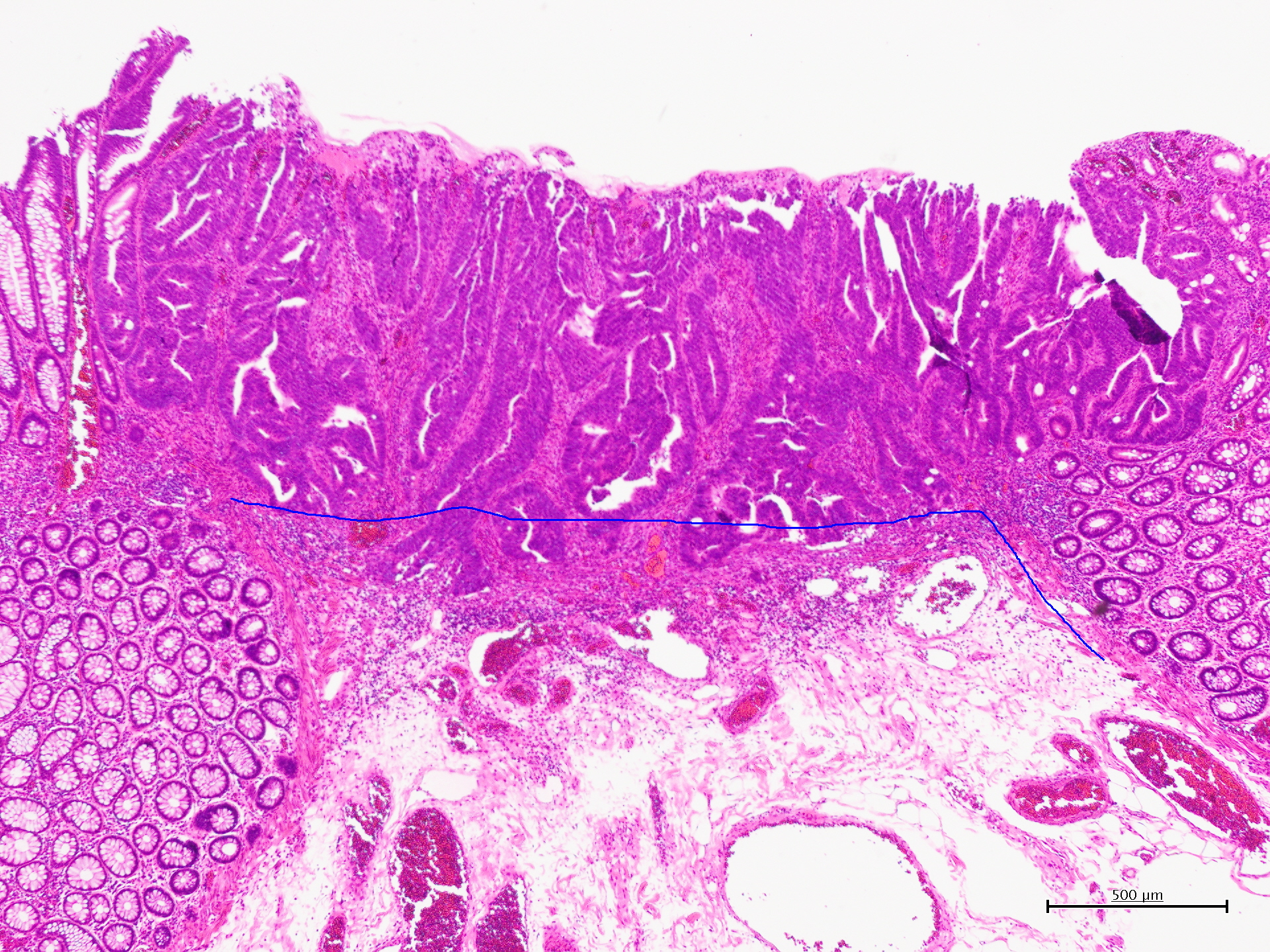
10. Pathological diagnosis
11. Pathological image
Case Video
Overall Comment
This case demonstrates a 10-mm rectal lesion (Rs) of macroscopic type 0-IIa+IIc, showing a superficially elevated component with a central depressed area. On white-light imaging, the lesion appeared slightly elevated with an irregular surface, while TXI improved visualization of both the overall contour and the depressed component. Indigo carmine chromoendoscopy clearly delineated the lesion margin and confirmed the depressed morphology. On NBI, the central part of the lesion was optically diagnosed as JNET Type 2B, whereas JNET Type 2A findings were also present at the lesion margin, suggesting coexistence of adenomatous tissue. Magnifying chromoendoscopy demonstrated a mildly irregular Kudo type Vi pit pattern in the central area, along with an invasive pattern-positive area measuring approximately 3~5 mm in width, while a type IV pit pattern was observed at the margin, raising suspicion of coexisting tubulovillous adenoma. Based on these findings, PAEM (peranal endoscopic myectomy) was performed. Histopathological examination confirmed adenocarcinoma (tub1) with tubulovillous adenoma, pT1a (SM 300 μm), BD1, ly0, v0, pHM0, and pVM0. R0 resection was achieved, and the patient is currently under follow-up. This highly educational case illustrates that even a small lesion can contain both invasive carcinoma and adenomatous components, emphasizing the importance of combined assessment of macroscopic type, depressed morphology, JNET classification, pit pattern heterogeneity, and appropriate therapeutic decision-making.
* Specifications, design and accessories are subject to change without any notice or obligation on the part of the manufacturer.